
Comment:
This 2017 article’s real contribution here isn’t the narrative review—which, as is too selective to be high-quality—but the new VICTOR-2 subgroup data. While a 35.7% Clinical Benefit Rate in an elderly (median age 69) metastatic TNBC population is certainly interesting, it’s from a tiny, single-arm cohort of 28 patients.
This paper highlights metronomic chemotherapy as a potential palliative option, especially for frail or elderly patients where standard, max-dose chemo is not a viable option due to toxicity.
Summary:
Clinical Bottom Line
This 2017 article by Cazzaniga et al. provides a narrative review of the sparse preclinical and clinical data available for metronomic chemotherapy (mCHT) in triple-negative breast cancer (TNBC). The authors conclude that while evidence is very limited—drawn mostly from small Phase II trials or subgroup analyses—some promising results exist, particularly as a potential treatment option for specific populations like the elderly.
Crucially, this paper is not a systematic review and its conclusions are based on a selective literature search. Its most novel contribution is the first-time reporting of prospective data from the TNBC subgroup (n=28) of the authors’ own VICTOR-2 Phase II trial, which showed a clinical benefit rate of 35.7% with a metronomic combination of vinorelbine and capecitabine.
Results
Metronomic chemotherapy is defined as the minimum biologically effective dose of a chemotherapy agent given continuously with no prolonged drug-free breaks. The review summarizes data across three setting1s:
Preclinical Data
-
One study in a TNBC mouse model found that metronomic topotecan combined with pazopanib significantly enhanced antitumor activity and prolonged survival compared to either drug alone.
(Neo)Adjuvant Setting
-
The review highlights mixed results from a few trials.
-
The IBCSG 22-00 trial found no statistically significant benefit for metronomic cyclophosphamide and methotrexate (CM) maintenance in the overall TNBC population.
-
In contrast, a study by Nasr et al. concluded that extended adjuvant metronomic CM did achieve a significant improvement in survival and was well-tolerated.
-
The authors of this review state their opinion that mCHT should not be adopted in the adjuvant setting without stronger preclinical data.
Metastatic Setting
-
Data is noted as being very scarce, with most trials enrolling HER2-negative patients and reporting on TNBC patients only in subgroup analyses.
VICTOR-2 Subgroup Analysis (New Data)
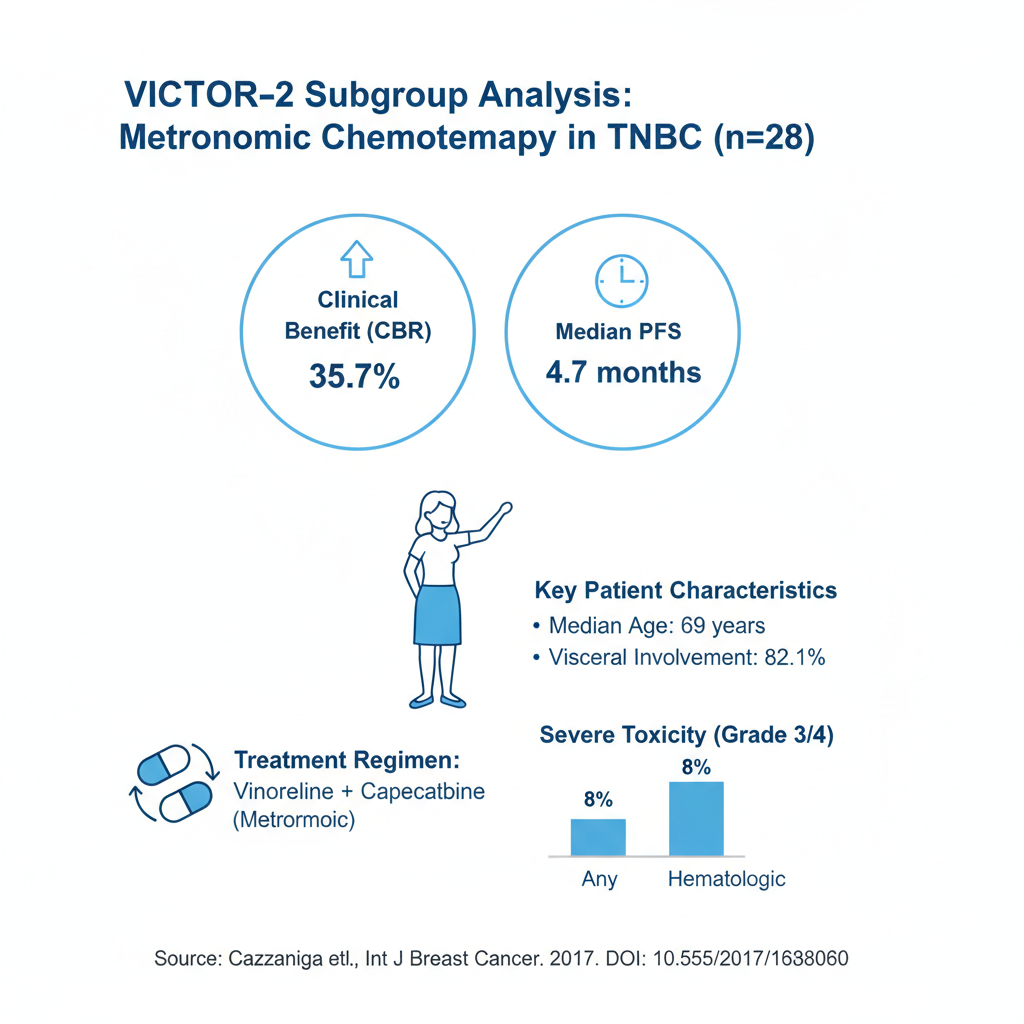
The review presents new data on 28 TNBC patients from the VICTOR-2 study, a Phase II, single-arm trial evaluating metronomic vinorelbine (40 mg three times/week) and capecitabine (500 mg three times/day).
-
Population: Median age was 69 years. 82.1% had visceral involvement.
-
Efficacy:
-
Clinical Benefit Rate (CBR): 35.7%
-
Disease Control Rate (DCR): 53.6%
-
Median PFS: 4.7 months
-
-
Toxicity: Severe (Grade 3/4) toxicity did not exceed 8% and was mainly hematologic.
Critical Appraisal
This article is a hybrid narrative review and primary data report. Its structure has significant limitations as a review.
-
Certainty of Evidence: The overall certainty of the evidence presented for mCHT in TNBC is Very Low. This rating is based on the review’s reliance on a small number of preclinical studies, subgroup analyses, and small, non-randomized Phase II studies.
-
Search Strategy & Reporting: The article does not follow PRISMA guidelines for systematic reviews.
-
Search Strategy: This is a significant limitation. The search was restricted to only one database (PubMed) using three keywords, creating a high risk of selection bias.
-
Bias Assessment: The authors do not provide a formal risk of bias assessment for the included studies.
-
-
Primary Contribution: The review itself is limited. The article’s most significant contribution is the inclusion of the first prospective data (though from a small, single-arm subgroup) on metronomic vinorelbine and capecitabine in metastatic TNBC patients.
Article Citation
-
Title: Metronomic Chemotherapy in Triple-Negative Metastatic Breast Cancer: The Future Is Now?
-
Authors: M. E. Cazzaniga, L. Cortesi, A. Ferzi, L. Scaltriti, F. Cicchiello, M. Ciccarese, S. Della Torre, F. Villa, M. Giordano, C. Verusio, M. Nicolini, A. R. Gambaro, L. Zanlorenzi, E. Biraghi, E. Casini, L. Legramandi, and E. Rulli
-
Journal: International Journal of Breast Cancer
-
Year: 2017
-
DOI: 10.1155/2017/1683060
Original Article:
Full text: PubMed Central
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.