
Comment:
This prospective cohort analysis provides a highly needed, long-term look at the structural reality of post-treatment life for breast cancer survivors. The central strength of the study is how it separates the distinct physical trajectories of cytotoxic chemotherapy from hormone-modulating endocrine therapies, balancing them against age-matched controls to account for the background baseline of normal aging.
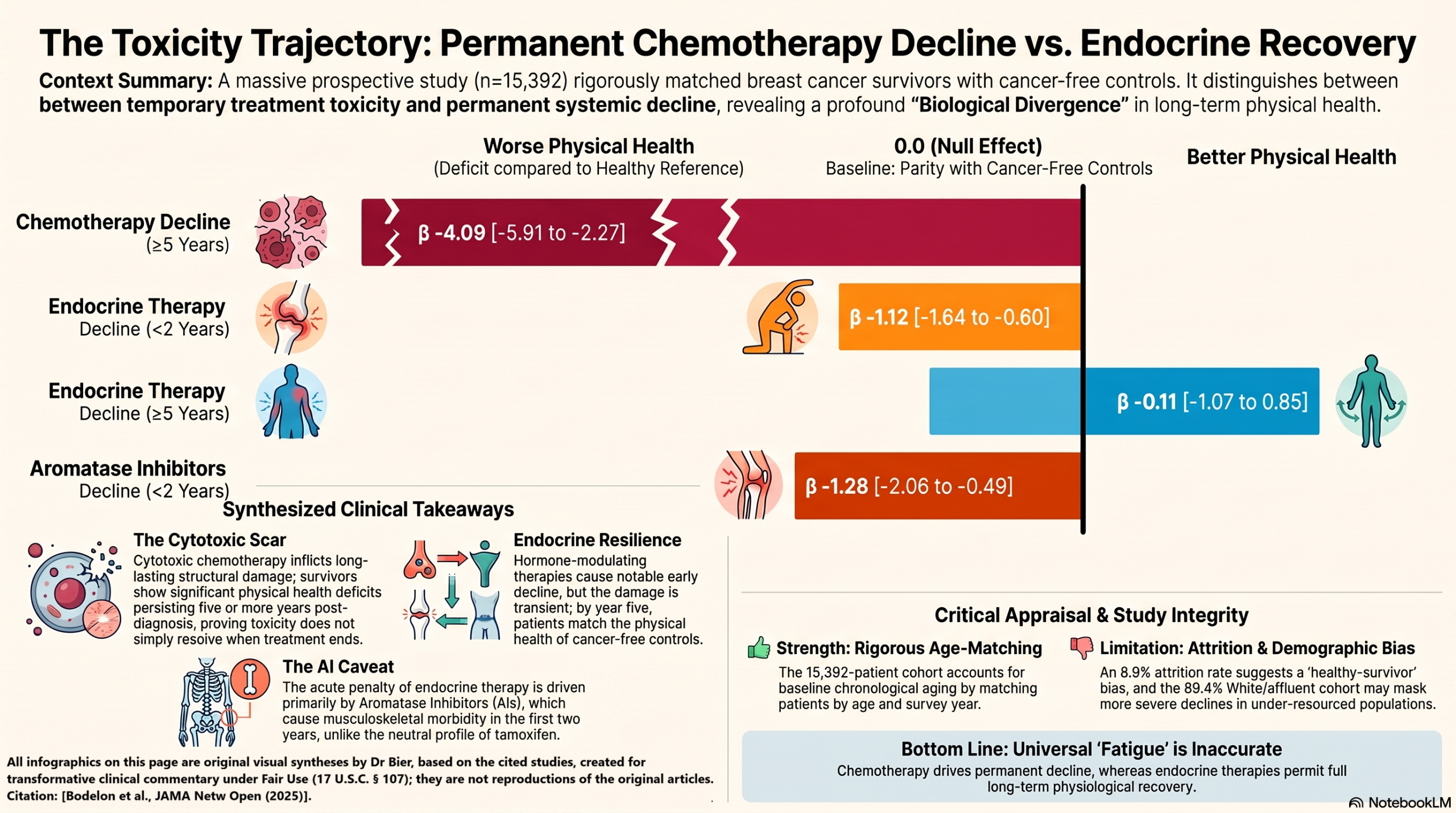
The Cytotoxic Baseline vs. Endocrine Resilience
The findings present a clear biological divergence. For patients undergoing chemotherapy, the physical health deficits are profound and long-lasting, remaining highly significant even at the $\ge 5$-year mark ($\beta = -4.09$ for chemo alone). This lingering deficit is entirely plausible given what we understand about the systemic, cell-level toll of cytotoxic agents and their tendency to accelerate aging phenotypes.
Conversely, the data for endocrine therapy alone offers a reassuring clinical signal. While there is an initial physical decline within the first two years post-diagnosis ($\beta = -1.12$), these patients structurally recover to match their cancer-free peers over the long term.
The Subtype Nuance: AI vs. Tamoxifen
What makes this study particularly sharp is the granular breakdown of the endocrine cohorts. The short-term physical health decline was not a universal class effect; it was almost entirely driven by patients receiving aromatase inhibitors (AIs) ($\beta = -1.28$ within 2 years), whereas the tamoxifen group showed no statistically significant deficit compared to controls at any interval. This aligns perfectly with clinical experience regarding AI-induced musculoskeletal symptoms and bone pain, which likely peak early on and are either proactively managed or adaptively tolerated over time.
The Observational Lens
As with any large-scale survey mapping quality-of-life metrics, we have to keep an objective “wait and see” perspective regarding unmeasured confounding. The authors note a modest attrition rate, where about 8.9% of survivors missed the final 2018 survey wave. It is highly possible that patients experiencing the most severe, unmanaged physical declines were the ones who dropped out, which could mean the long-term survival metrics are slightly shielded by a subtle healthy survivor effect. Additionally, the cohort’s baseline demographics skew toward a higher socioeconomic and educational profile, meaning these women likely had optimal access to supportive care interventions to buffer their physical recovery.
Takeaway
Ultimately, these findings provide high-value longitudinal insights that help us move past generalized assumptions about “post-cancer fatigue.” It gives clinicians a clear, data-driven map to counsel patients on what to realistically expect: a temporary, manageable hurdle for endocrine regimens—particularly AIs—versus a prolonged, systemic recovery window for cytotoxic chemotherapy. It underscores the necessity of designing proactive, early physical interventions specifically tailored to the unique metabolic and structural demands of each treatment pathway.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This prospective observational cohort study demonstrates a distinct, treatment-dependent trajectory for physical health decline in breast cancer survivors compared to normal aging controls. While both chemotherapy and endocrine therapy are associated with an initial physical health decline within the first 2 years post-diagnosis, the decline is long-lasting (persisting beyond 5 years) only in women who received chemotherapy. Conversely, survivors treated with endocrine therapy alone typically see their physical health recover to match age-matched cancer-free controls after 2 years.
As an observational study, these findings identify strong adjustments and associations but cannot prove direct causation due to potential unmeasured confounding or the lack of randomized treatment allocation. However, it offers high-value longitudinal insights to help clinicians counsel patients on survivorship expectations and proactively manage treatment sequelae.
Results in Context
Main Results
The study compared patient-reported physical health trajectories across different therapeutic arms against age-matched controls over multiple time intervals:
- Within 2 Years of Diagnosis: Significant declines in physical health were observed across all active treatment groups compared to controls. The chemotherapy-containing regimens demonstrated the most profound drops.
- Beyond 2 Years Post-Diagnosis: The physical health of women who received endocrine therapy alone stabilized and became statistically indistinguishable from women without cancer. In contrast, the deficit persisted significantly for those who underwent chemotherapy.
- Endocrine Therapy Subtypes: The short-term decline within the endocrine group was entirely driven by aromatase inhibitors (AIs). Survivors taking tamoxifen did not experience a significant physical health decline compared to controls at any time point.
The primary longitudinal findings are summarized below in terms of the adjusted \beta coefficients (with 95% Confidence Intervals) representing the physical health score change relative to cancer-free controls:
|
Treatment Category |
Before Diagnosis (β) |
<2 Years Post-Diagnosis (β) |
2 to <5 Years Post-Diagnosis (β) |
≥5 Years Post-Diagnosis (β) |
|
No Chemo / No Endocrine |
-0.10 (-1.15 to 0.95) |
-1.10 (-1.99 to -0.21) |
-0.70 (-1.56 to 0.16) |
0.18 (-1.21 to 1.59) |
|
Endocrine Therapy Alone |
-0.19 (-0.77 to 0.40) |
-1.12 (-1.64 to -0.60) |
-0.40 (-0.94 to 0.14) |
-0.11 (-1.07 to 0.85) |
|
Chemotherapy Alone |
-0.65 (-1.93 to 0.62) |
-3.13 (-4.19 to -2.06) |
-1.20 (-2.32 to -0.07) |
-4.09 (-5.91 to -2.27) |
|
Chemo + Endocrine |
0.17 (-0.68 to 1.03) |
-3.26 (-3.97 to -2.55) |
-1.34 (-2.07 to -0.61) |
-1.65 (-2.85 to -0.46) |
Statistical Definitions
The beta coefficient in this linear regression analysis represents the adjusted mean difference in the PROMIS physical health T-score between the breast cancer survivor subgroup and the age-matched cancer-free control group. A negative \beta value signifies worse physical health relative to the reference population, accounting for standard aging trajectories.
Study Participants & Attrition Flow
- Total Cohort: 15,392 women (2,566 diagnosed with nonmetastatic breast cancer; 12,826 age-matched controls).
- Survey Completion: 2,161 breast cancer survivors (84.2%) returned all three longitudinal surveys.
- Missing Data/Exclusions: 273 women (10.6%) returned only the baseline and 2018 surveys. Notably, 132 women (5.1%) returned only the baseline and 2018 surveys, while 273 women (10.6%) returned only the baseline and 2015 surveys.
Assertive Critical Appraisal
Limitations & Bias (STROBE Assessment)
- Exposure Information Limitations: The data were limited to first-line treatment broad categories. The investigators lacked granular data regarding specific chemotherapy agents, dosages, targeted biological therapies (e.g., anti-HER2 agents), or immunotherapies, which may impact physical health uniquely.
- Potential Attrition Bias: There is a notable 8.9% drop-out rate between post-diagnosis survey intervals. If this missingness was non-random (i.e., women with the worst physical health or highest treatment toxicity failed to return follow-up surveys), the study would suffer from a healthy-survivor bias, artificially underestimating the true magnitude of long-term physical decline.
- Adherence Unavailability: Longitudinal adherence or non-adherence to the prescribed 5-to-10-year endocrine therapy regimens was not tracked. This prevents an analysis of whether the physical recovery seen in the endocrine arm after 2 years was due to symptom adaptation or early treatment discontinuation.
Reporting Quality Assessment (STROBE)
The study demonstrates high reporting quality against the STROBE statement checklist. Crucially, the authors explicitly described their extensive efforts to address potential sources of confounding. The primary models were properly adjusted for matching factors (age, time from diagnosis) and body mass index (BMI). Furthermore, they conducted robust sensitivity models additionally adjusting for smoking status, alcohol consumption, diabetes, and hypertension, which yielded identical results and confirmed the stability of the primary findings.
Routinely Collected Health Data (RECORD)
While this study utilized data linkage to state cancer registries to confirm first-course treatments and cancer staging, it fundamentally relies on an active, prospective research cohort (CPS-3) rather than purely passive administrative electronic health records or insurance claims data. The authors adequately detailed the high agreement (85.0% to 99.4%) between the registry data and patient self-reports, satisfying the structural transparency required for registry-linked real-world data.
Applicability
The generalizability of these findings to a broader clinical practice is significantly constrained by a healthy, affluent user bias. The study population was predominantly non-Hispanic White (89.4%) and possessed higher education and income levels than national US averages. In a standard clinical setting, underserved minority populations with higher baseline comorbidities and fewer supportive resources may experience more severe or prolonged physical health declines than documented here.
Research Objective
The study aimed to evaluate long-term physical health decline trajectories among breast cancer survivors by treatment received (chemotherapy, endocrine therapy, or both) relative to a reference population of age-matched women without a history of cancer.
Study Design
This was a prospective, observational, matched cohort study. Breast cancer survivors were dynamically matched in a 1:5 ratio with cancer-free controls based on age (\pm2 years) and the specific year of survey return (\pm1 year) to control for the baseline natural effects of normal chronological aging.
Setting and Participants
- Setting: A large-scale, prospective US community-based framework utilizing the American Cancer Society’s Cancer Prevention Study-3 (CPS-3) across 35 states, the District of Columbia, and Puerto Rico.
- Timeline: Participant enrollment occurred between 2006 and 2013, with longitudinal health surveys collected at baseline, 2015, and 2018; follow-up for this analysis extended through April 1, 2020.
- Eligibility Criteria: Female participants aged 30 to 65 years at enrollment with no prior history of cancer. To be included as a case, women must have developed a verified first primary incident nonmetastatic breast cancer and returned a post-diagnosis survey at least 90 days after diagnosis. Patients with distant metastasis at diagnosis or those who did not undergo primary surgery for invasive disease were excluded.
Bibliographic Data
- Title: Physical Health Decline After Chemotherapy or Endocrine Therapy in Breast Cancer Survivors
- Authors: Clara Bodelon, Matthew Masters, Den E. Bloodworth, Peter J. Briggs, Erika Rees-Punia, Lauren E. McCullough, Alpa V. Patel, Lauren R. Teras
- Journal: JAMA Network Open
- Year: 2025
- DOI: 10.1001/jamanetworkopen.2024.62365
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.