
Comment:
There is a pervasive habit in oncology of treating supportive care medications as biologically inert. However, outside of the cancer clinic, the epidemiological data is already glaringly clear: proton pump inhibitors (PPIs) are not benign. Chronic PPI use is definitively linked to increased risks of chronic kidney disease, major adverse cardiovascular events, and elevated all-cause mortality.
This post-hoc analysis of the PACIFIC trial brings that systemic cost directly into our wheelhouse, demonstrating that the biological damage of PPIs extends far beyond vascular and renal toxicity—they appear to actively interfere with immunotherapies.
The Oncologic Penalty
When we apply the core principle of informed medicine, we have to assume the biological risk presented in this data is accurate. And the penalty here is staggering. In patients receiving consolidation durvalumab for stage III NSCLC, baseline exposure to PPIs slashed median Overall Survival from 57.9 months down to 33.0 months (HR 1.66). We are looking at a nearly two-year survival deficit associated with OTC acid blockers. We shouldn’t view these as passive supportive agents; they are active biological variables that effectively disarm the PD-L1 blockade.
The Placebo Validation
What makes this biological penalty so convincing—and what pushes us past the usual “confounding by indication” dismissals—is the placebo group.
If this survival drop were simply a reflection of baseline frailty—arguing that patients taking PPIs were just sicker, suffering from worse radiation esophagitis, and destined to do poorly—we would expect to see a parallel survival drop in the placebo arm. We didn’t. In the placebo group, PPI exposure was not associated with changes in progression-free or overall survival. This strongly suggests a true, treatment-dependent interference: the microbiome disruption specifically neutralizes the durvalumab.
Takeaway
This data requires us to elevate our suspicion index for the downstream consequences of supportive prescriptions. PPIs are not benign antacids; they are serious systemic interventions. As Naturopathic Oncologists, we have many options that can help without resorting to potentially dangerous options.
Summary:
Clinical Bottom Line: This study suggests that baseline exposure to proton pump inhibitors (PPIs) and systemic antibiotics diminishes the efficacy of consolidation durvalumab in patients with unresectable stage III non-small-cell lung cancer (NSCLC). However, because this is a post-hoc, observational analysis of a randomized trial, these findings cannot prove causation. The results should be viewed with caution due to the high risk of confounding by indication, meaning the underlying conditions requiring PPIs or antibiotics may be driving the poorer survival outcomes rather than the medications themselves.
Results in Context
- Primary Outcome:
- The co-primary endpoints evaluated were progression-free survival (PFS) and overall survival (OS).
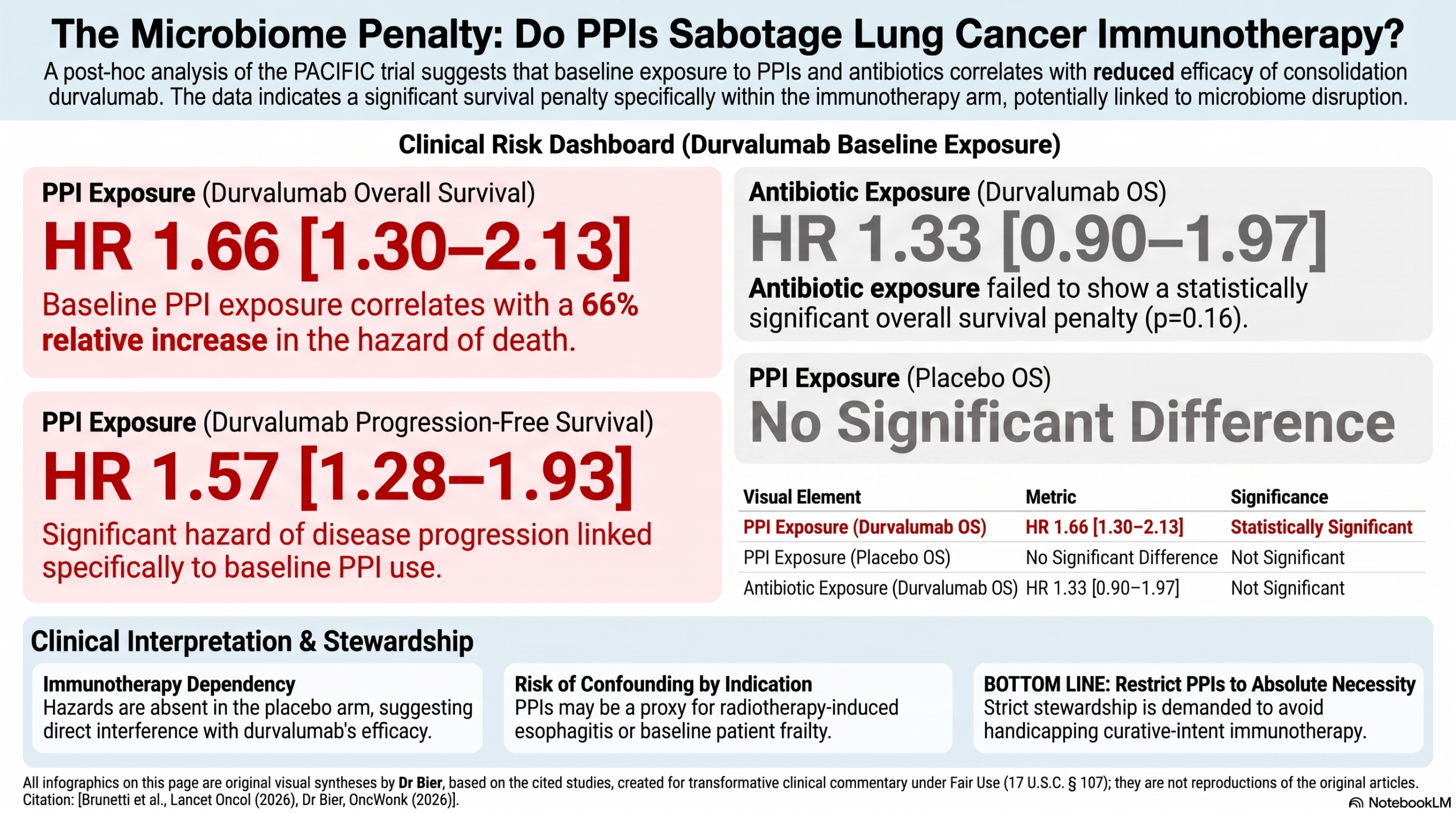
- In the durvalumab group, baseline exposure to PPIs was associated with a significantly shorter PFS (9.4 months vs 17.2 months; Hazard Ratio [HR] 1.57) and a shorter OS (33.0 months vs 57.9 months; HR 1.66) compared to patients with no PPI exposure.
- A hazard ratio of 1.66 means there was a 66% relative increase in the hazard of death in the PPI-exposed group compared to the unexposed group.
- Baseline exposure to antibiotics in the durvalumab group was associated with a shorter PFS (9.2 months vs 15.6 months; HR 1.50) compared to no antibiotic exposure.
- However, antibiotic exposure was not associated with a statistically significant change in OS (37.7 months vs 49.2 months; HR 1.33, p=0.16).
- In the placebo group, neither PPI nor antibiotic exposure was significantly associated with changes in PFS or OS.
- Key Secondary & Specialized Outcomes:
- Oncology Endpoints & Response Criteria:
- The primary endpoints were OS and PFS.
- Overall Survival is the most reliable endpoint for demonstrating a true clinical benefit to patients.
- Progression-Free Survival is a surrogate endpoint; while these endpoints can be measured sooner than OS, an improvement in a surrogate endpoint does not always translate to patients living longer.
- Disease progression in this trial was assessed according to Response Evaluation Criteria in Solid Tumors (RECIST), version 1.1.
- RECIST 1.1 is the standard set of anatomical criteria used to define and measure tumor response and progression in clinical trials.
- Harms and Adverse Events:
- Because the assessment of harms was not an objective of this specific post-hoc analysis, no formal between-group statistical comparisons of safety outcomes were performed.
Assertive Critical Appraisal
- Risk of Bias (RoB 2 Framework):
- The overall risk of bias for the specific associations evaluated in this paper is High.
- While the parent PACIFIC trial was a well-designed, randomized, double-blind study, this specific evaluation is a post-hoc observational analysis based on baseline medication exposure.
- Medication exposure (PPIs and antibiotics) was not a randomized variable.
- This introduces a critical risk of confounding by indication; the clinical conditions that prompted the prescription of PPIs (e.g., radiotherapy-related esophagitis) or antibiotics (e.g., infections, baseline frailty) could independently be responsible for the poorer outcomes observed.
- Subgroup Analyses:
- This study evaluates outcomes based on exposure to specific medications, effectively functioning as a subgroup analysis.
- Subgroup claims are often unreliable and should be viewed with skepticism unless the effect is large, highly statistically significant, pre-specified, and biologically plausible.
- This analysis was an exploratory, post-hoc evaluation that was not prespecified in the original trial protocol, which heavily limits the credibility of its claims.
- Reporting Quality Assessment (CONSORT):
- The paper includes a participant flow diagram (Figure 1) detailing the inclusion and exclusion of patients for this specific post-hoc analysis.
- However, the paper fails to adequately describe the methods for sequence generation and allocation concealment within this text, referring the reader instead to the parent trial publication for those critical methodological details.
- Applicability:
- The findings are highly relevant to clinical practice, as PPIs and antibiotics are commonly prescribed supportive medications for patients undergoing chemoradiotherapy for NSCLC.
- However, because of the observational nature of these findings, clinicians should not withhold clinically indicated supportive therapies based solely on these data.
- Research Objective:
- To assess the association of baseline exposure to antibiotics and proton pump inhibitors with progression-free survival and overall survival in patients with unresectable stage III NSCLC.
- Study Design:
- This was a post-hoc analysis of the PACIFIC trial, which was a randomized, double-blind, placebo-controlled phase 3 trial.
- Patients were randomly assigned in a 2:1 ratio to receive durvalumab or a matched placebo.
- This post-hoc analysis included 660 patients: 449 treated with durvalumab and 211 treated with placebo.
- Setting and Participants:
- Participants were enrolled globally between May 9, 2014, and April 22, 2016.
- Eligible patients were 18 years or older with histologically or cytologically documented unresectable stage III squamous or non-squamous NSCLC.
- Patients were required to have a WHO performance status of 0 or 1 and to have experienced no disease progression after completing at least two cycles of concurrent platinum-based chemoradiotherapy.
Bibliographic Data
- Title: Differential impact of proton pump inhibitors and antibiotics on immunotherapy efficacy after chemoradiotherapy in locally advanced non-small-cell lung cancer: a post-hoc analysis of the PACIFIC trial
- Authors: Leonardo Brunetti, Valentina Santo, David J Pinato, Fabrizio Citarella, Sarah Orlando, Fabian Acker, Vittoria Colella, Biagio Ricciuti, Jarushka Naidoo, Amin Nassar, Heather A Wakelee, Kazuki Takada, Abdul Rafeh Naqash, Marina C Garassino, Carlo Greco, Sara Ramella, Francesco Pantano, Giuseppe Tonini, Bruno Vincenzi, Bryan Arlunno, Jordi Remon, Claudia Parisi, David Planchard, Benjamin Besse, Antoine Desilets, Bertrand Routy, Arielle Elkrief, Fabrice Barlesi, Lisa Derosa, Alessio Cortellini
- Journal: The Lancet Oncology
- Year: 2026
- DOI: https://doi.org/10.1016/S1470-2045(26)00191-9
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.