
Comment:
We naturally want screening to work because catching pathology early has an undeniable intuitive appeal. However, the structural reality of observational studies keeps showing us the same outcome. This study is a perfect case in point. It elegantly uses negative controls to expose how easily Healthy User Bias can manufacture a massive, completely artificial survival benefit.
The Mirage of Off-Target Protection
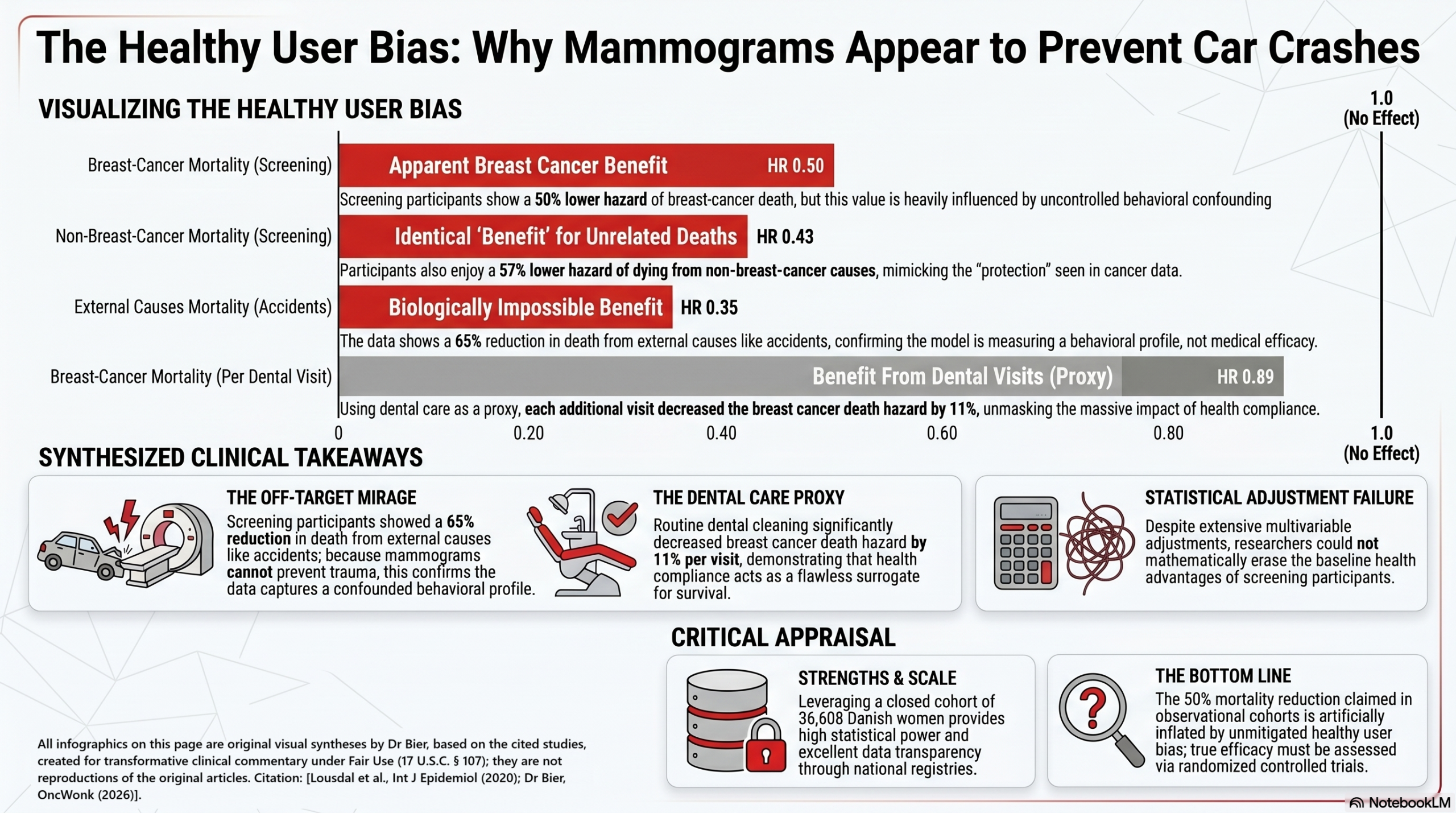
The dataset tracks 36,608 Danish women and shows that screening participants enjoyed an impressive-looking 50% lower hazard of breast-cancer death (HR 0.50; 95% CI 0.34, 0.74) even after adjusting for classic socioeconomic variables.
The fascinating part of this paper is what happens when the authors look at outcomes that a mammogram could not possibly influence biologically. They found that these exact same screening participants also experienced a 57% lower hazard of dying from non-breast-cancer causes (HR 0.43) and an incredible 65% lower hazard of dying from external causes like accidents or assaults (HR 0.35; 95% CI 0.23, 0.54).
Unless we believe that stepping inside a mammography suite alters a patient’s driving habits or protects them from physical trauma, the model isn’t measuring clinical efficacy. It’s capturing a behavioral profile. The authors flip the equation and demonstrate this by tracking dental care as a negative-control exposure. Women who routinely saw a dentist had a point estimate suggesting a 25% reduction in breast-cancer mortality (HR 0.75), though the 95% CI just nicks the null line at 0.56–1.01.
However, the true statistical confirmation lands when you look at their continuous dose-response model: each additional dental visit significantly decreased the hazard of breast-cancer death by 10% to 11% (HR 0.89; 95% CI: 0.82–0.96), completely independent of whether they ever had a mammogram. Showing up for routine scaling is acting as a flawless surrogate marker for a highly compliant, risk-averse individual who is less likely to die from anything.
A Systemic Pattern, Not an Isolated Flaw
This isn’t a quirk unique to the Danish registries; it is a systemic feature of observational screening cohorts. When we look at macro-level data, like the landmark Autier et al. (2024) meta-analysis, the exact same statistical mirror appears.
Across millions of women in 18 cohort studies, Autier found that screening attendees had a summary relative risk (SRR) of 0.55 for breast cancer mortality, alongside an almost identical SRR of 0.54 for all-cause mortality. When tracked head-to-head within the same cohorts, the apparent drop in breast cancer death (SRR 0.63) was statistically indistinguishable from the drop in completely unrelated, off-target deaths (SRR 0.54). Standard multivariable adjustments completely fail to clean this up.
The Takeaway
When a screening tool repeatedly implies that it protects women from car crashes, strokes, and dental neglect at the exact same rate it protects them from tumor mortality, we are looking at a self-selection artifact.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This study demonstrates that the approximately 50% reduction in breast-cancer mortality often seen in observational studies of mammography screening is likely a significant overestimate driven by “healthy user bias” (uncontrolled confounding). By using negative controls—outcomes like accidental death that cannot biologically be affected by a mammogram—the researchers found that screening participants were inherently “protected” against almost everything, including causes totally unrelated to cancer. This implies that participants and non-participants are fundamentally different at baseline in ways that standard statistical adjustments cannot fully fix. For the clinician, this means observational data comparing “screened” vs. “unscreened” women likely reflects the better health behaviors of the participants as much as, if not more than, the efficacy of the screening itself.
Results in Context
- Main Results (Breast-Cancer Mortality): Screening participants had a 53% lower hazard of breast-cancer death in unadjusted models (HR 0.47; 95% CI 0.32, 0.69). After adjusting for education, income, parity, and hormone use, the hazard remained 50% lower (HR 0.50; 95% CI 0.34, 0.74).
- Negative-Control Outcomes: Screening participants also had a 57% lower hazard of death from causes other than breast cancer (HR 0.43; 95% CI 0.39, 0.46) and a 65% lower hazard of death from external causes like accidents or assaults (HR 0.35; 95% CI 0.23, 0.54).
- Negative-Control Exposure: Women who participated in dental care (a proxy for healthy behavior) had a 25% lower hazard of breast-cancer death (HR 0.75; 95% CI 0.56, 1.01), regardless of whether they actually had a mammogram.
- Definitions: A Hazard Ratio (HR) of 0.50 indicates that, at any given time, the “exposed” group had half the risk of death compared to the “unexposed” group. Negative controls are tools used to detect bias; if an intervention appears to “prevent” an unrelated outcome (like a mammogram preventing a car accident), it indicates the presence of confounding.
- Participants: The study included 36,608 Danish women aged 50–52 years who were invited to a mammography program.
Assertive Critical Appraisal
- Limitations & Bias (STROBE Framework): The central finding is the presence of healthy user bias (or compliance bias). Because mammography is voluntary, women who choose to participate often have higher socioeconomic status, better health literacy, and engage in other preventive behaviors (like dental visits). The study proves that even with high-quality registry data, we cannot “adjust away” these baseline differences.
- Reporting Quality Assessment (STROBE): The authors provide a robust description of their efforts to address confounding. The use of negative controls is a sophisticated method to expose the “invisible” bias inherent in observational screening data.
- Reporting Quality Assessment (RECORD): As a study using Real-World Data from Danish national registries, it excels in data transparency. They clearly defined data sources for cancer (Danish Cancer Registry), deaths (Register of Causes of Death), and socioeconomic factors (Statistics Denmark). Participant selection and “mimicked” follow-up dates for non-participants were logically handled and tested for robustness.
- Applicability: These findings suggest that many observational studies claiming massive benefits for mammography are likely confounded. Clinicians should rely more heavily on randomized controlled trials (RCTs) for efficacy estimates, as RCTs eliminate this healthy user bias through random assignment.
Research Objective
To evaluate the extent of uncontrolled confounding in observational studies of mammography screening by using negative-control exposures and outcomes.
Study Design
A closed cohort study using comprehensive Danish national registries. Exposure (screening participation) was determined during the second round of invitations to ensure all included women had at least one “clean” initial screen, reducing “healthy-start” bias.
Setting and Participants
- Location: Copenhagen and Funen, Denmark.
- Timeframe: 1991 through 2001 (invitation) with follow-up until 2014.
- Eligibility: Women aged 50–52 years at first invitation with no prior breast cancer who participated in their first screening round and received a normal result.
Bibliographic Data
- Title: Negative controls to detect uncontrolled confounding in observational studies of mammographic screening comparing participants and non-participants
- Authors: Mette Lise Lousdal, Timothy L Lash, W Dana Flanders, M Alan Brookhart, Ivar Sønbø Kristiansen, Mette Kalager, and Henrik Støvring
- Journal: International Journal of Epidemiology
- Year: 2020
- DOI: 10.1093/ije/dyaa029
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.