
Comment:
I’ve always advocated that screening needs to prove actual survival efficacy, not just give us the illusion of control. We want screening to work because catching pathology early has an undeniable intuitive appeal, but as we’ve seen across numerous papers, observational designs claiming that screening saves lives are frequently built on statistical quicksand. This study is a perfect case in point. It cleanly exposes how a popular observational evaluation model can manufacture a significant finding when one isn’t there.
The Screening Mirage vs. Structural Reality
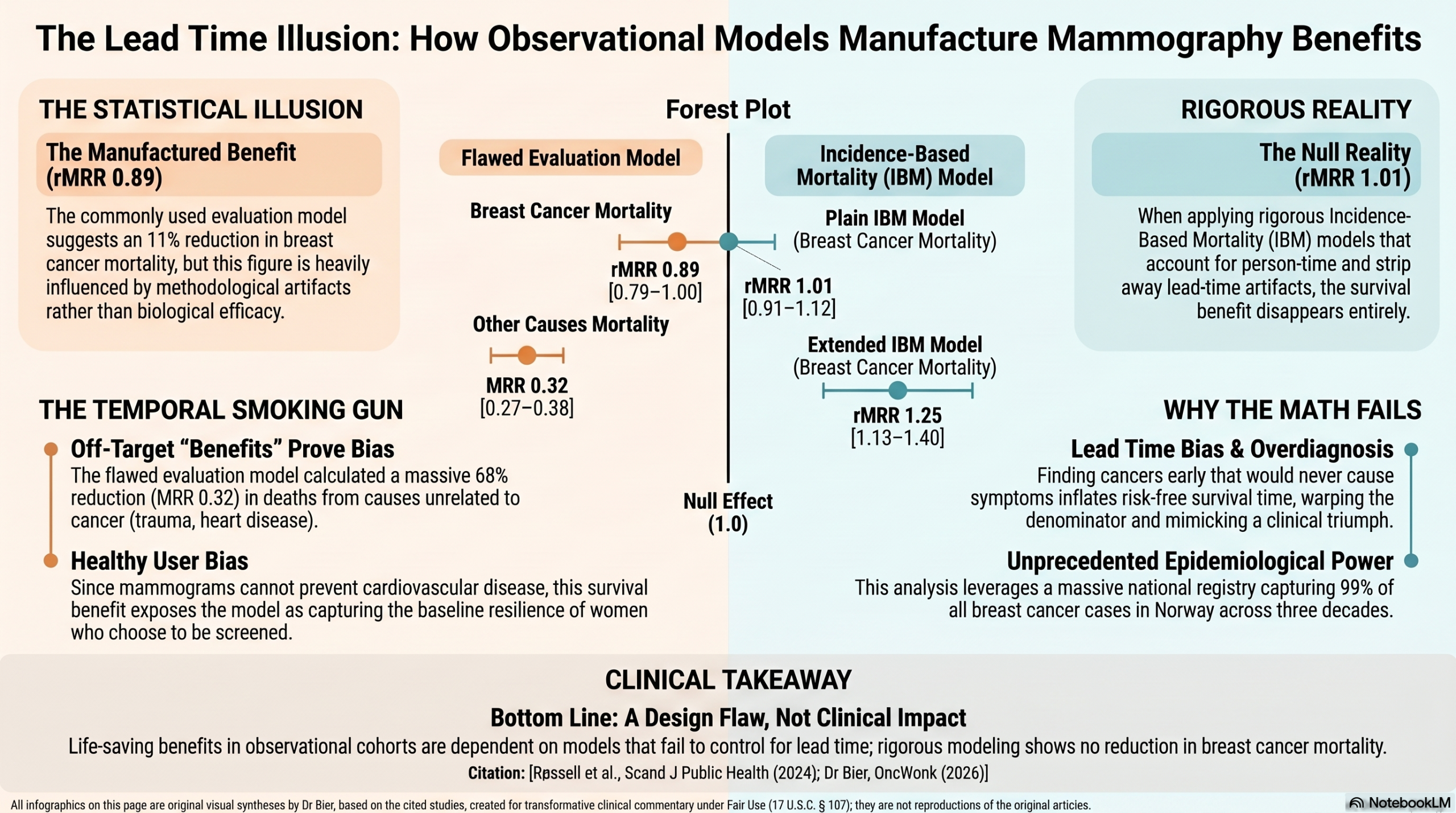
When the researchers tracked the Norwegian mammography data using a commonly accepted evaluation model, it yielded a seemingly impressive 11% reduction in breast cancer mortality (rMRR = 0.89). But when they stripped away the methodological artifacts using more traditional Incidence-Based Mortality (IBM) models designed to handle person-time cleanly, that survival benefit completely vanished. The traditional models showed no significant mortality reduction at all.
The study beautifully demonstrates how lead time bias and overdiagnosis warp the math. The model frequently used in mammography observational studies restrict follow-up after the screening age only to women diagnosed during the screening period, which floods the screening cohort with risk-free person-time that makes it look like there’s an advantage.
The Temporal Smoking Gun
The smoking gun in this paper is the temporal trend signal. The frequently used flawed evaluation model also calculated a 68% reduction in mortality from other causes (MRR = 0.32) among the screening-eligible women. Unless mammograms possess a biological mechanism that magically prevents cardiovascular disease, strokes, and car accidents, the model is clearly capturing a statistical artifact—a healthy user reflection—rather than a true screening effect.
This isn’t an isolated flaw unique to Norway; it’s a structural feature of observational screening cohorts. In a comprehensive 2024 systematic review and meta-analysis published in the Journal of Clinical Epidemiology, Autier et al. (2024) tracked millions of women across 18 cohort studies and uncovered a staggering parallel. They found that women attending screening had a summary relative risk (SRR) of 0.55 for breast cancer mortality, but an almost identical SRR of 0.54 for all-cause mortality.
Even more telling, in the studies that tracked both outcomes head-to-head within the same identical cohorts, the apparent risk reduction for breast cancer death (SRR 0.63) was statistically indistinguishable from the reduction in completely unrelated, off-target deaths (SRR 0.54).
Because a mammogram cannot alter the trajectory of non-cancerous diseases or accidental trauma, these off-target survival benefits serve as the ultimate proof of Healthy User Bias. We aren’t measuring the clinical efficacy of universal screening; we are merely documenting the baseline resilience, lower risk profiles, and health literacy of the women who choose to show up for the scans.
Takeaway
When an observational framework requires this much statistical contortion to show a benefit—and repeatedly implies that the intervention prevents non-cancer deaths along the way—we are looking at a design flaw, not a clinical impact. When we look at randomized controlled trials (review here) where this self-selection artifact is removed, the impact on all-cause mortality is entirely flat. Until the data moves the needle on true overall survival, we must recognize that the “life-saving” benefits often touted in cohort designs are almost certainly health user bias and not true screening effect.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This study demonstrates that the “evaluation model” used in several high-profile reports likely overestimates the mortality benefits of mammography screening due to significant lead time bias and overdiagnosis. While this specific model suggested an 11% reduction in breast cancer mortality, two traditional incidence-based mortality (IBM) models—designed to exclude these biases—found no significant mortality benefit from the Norwegian screening program. Clinicians should interpret observational screening evaluations with caution, as methodological choices regarding follow-up and person-time inclusion can create a “pseudo-effect” where none exists.
Results in Context
Main Results
- Evaluation Model (Weighted): Found a relative mortality rate ratio (rMRR) of 0.89 (95% CI 0.79–1.00), implying an 11% reduction in breast cancer mortality.
- Plain IBM Model: Found an age-adjusted rMRR of 1.23 (95% CI 1.08–1.40) when comparing eligible women to younger ineligible women, and 1.01 (95% CI 0.91–1.12) when comparing to older ineligible women.
- Extended IBM Model: Found an age-adjusted rMRR of 1.25 (95% CI 1.13–1.40).
- Bias Impact: The 11% reduction in the evaluation model was driven by a massive reduction estimate (MRR = 0.12) specifically in the period after screening age, where person-time was restricted only to those diagnosed during screening.
Definitions
- Incidence-Based Mortality (IBM): A measure that only counts breast cancer deaths among women diagnosed after their first invitation to screening, ensuring that “pre-existing” cancers do not dilute or bias the results.
- Relative Mortality Rate Ratio (rMRR): A “difference-in-difference” estimate. It compares the change in mortality in the screening group to the change in mortality in an unscreened control group over the same periods.
- Lead Time Bias: A bias occurring when screening moves the date of diagnosis forward in time without actually delaying the date of death, making “survival” appear longer simply because the clock started earlier.
Participants
- The study utilized registry data for the entire female population of Norway across 19 counties from 1986 to 2016.
- The total number of breast cancer deaths included across models ranged from 5,394 to 7,608.
Assertive Critical Appraisal
Limitations & Bias (STROBE Framework)
- Methodological Lead Time Bias: The “evaluation model” restricted follow-up after screening age only to women diagnosed with breast cancer during the screening age. This creates a bias because an ineligible woman diagnosed after the “accrual period” contributes no person-time, whereas a screened woman whose diagnosis was moved earlier (lead time) contributes significant person-time at risk.
- Overdiagnosis Inflation: Women who are “overdiagnosed” (cancers found by screening that would never have caused symptoms or death) contribute exclusively “risk-free” person-time to the evaluation model, further underestimating mortality.
- Healthy User / Temporal Trends: A supplementary analysis revealed that mortality from other causes was also 68% lower in the evaluation model for eligible women (MRR = 0.32), suggesting that the model captures general health improvements and person-time accrual rather than a specific screening effect.
Reporting Quality Assessment (STROBE)
- The authors clearly describe efforts to address confounding by using a difference-in-difference approach, comparing eligible women to younger and older ineligible age groups to control for improvements in treatment and patient management over time.
Reporting Quality Assessment (RECORD)
- Data Sources: Explicitly described (Cancer Registry of Norway for clinical data; Statistics Norway for population data).
- Participant Selection: Clearly defined based on birth cohort, residence, and screening implementation dates in each county.
- Variable Definition: Exposures (screening eligibility) and outcomes (IBM deaths) are well-defined and adjusted for the month of implementation to avoid classification errors.
Applicability
- The findings are highly applicable to current debates regarding the efficacy of mammography. It suggests that reported 20% mortality reductions in previous observational studies using similar “evaluation models” may be largely due to methodological artifacts rather than clinical benefit.
Research Objective
To investigate potential lead time bias in the specific evaluation model (using restricted extended follow-up) compared with traditional IBM models when assessing the effect of mammography screening on breast cancer mortality.
Study Design
A population-based open cohort study using three distinct analysis models (Plain IBM, Extended IBM, and the Beau/Nyström Evaluation model) to compare incidence-based mortality before and after screening implementation.
Setting and Participants
- Setting: All 19 counties in Norway.
- Period: 1986–2016.
- Groups: Eligible women (aged 50–69) and ineligible control groups (younger < 50; older > 70/75).
Bibliographic Data
- Title: Evaluating mammography screening in observational cohort designs: the importance of avoiding lead time bias
- Authors: Eeva-Liisa Røssell, Mette Lise Lousdal, Jakob H. Viuff, Henrik Støvring
- Journal: Scandinavian Journal of Public Health
- Year: 2024
- DOI: 10.1177/14034048241288136
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.