
Comment:
The traditional clinical focus on “detecting cancer early” ignores the underlying reality that “saving a life from breast cancer” in a cohort study does not equate to “lengthening that patient’s life” in a randomized trial. This comprehensive meta-analysis highlights a persistent survival paradox: while cohort studies suggest massive benefits, the randomized controlled trials (RCTs)—where self-selection is removed—show zero impact on all-cause mortality.
This 2024 systematic review in the Journal of Clinical Epidemiology deconstructs the evidence to reveal a staggering truth: women who attend screening have an nearly identical reduction in risk for both breast cancer mortality and deaths from causes completely unrelated to the intervention, such as accidents or non-cancerous diseases. Because mammography has no biological mechanism to prevent a car crash or a stroke, these findings confirm that the perceived “survival benefit” is actually a marker of Healthy User Bias. For years, I have cautioned that we are measuring the baseline resilience of health-conscious women rather than the efficacy of the screening itself. Overall survival remains the only objective measure, and when we rely on observational data that fails to move the needle on all-cause mortality in randomized settings, we are merely documenting a self-selection artifact.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This systematic review and meta-analysis provides a critical reality check for observational data on breast cancer screening. It demonstrates that women who attend mammography have an nearly identical reduction in risk for both breast cancer mortality and deaths from causes completely unrelated to breast cancer (e.g., accidents, other diseases). Because mammography has no biological mechanism to prevent non-breast cancer deaths, these findings suggest that the perceived “survival benefit” in cohort studies is largely an artifact of healthy user bias—where health-conscious, resourceful women are more likely to get screened and more likely to live longer regardless of the intervention. Clinicians should rely on randomized controlled trials (RCTs), which show a breast cancer-specific benefit but no impact on all-cause mortality, rather than observational studies which appear to overestimate screening’s effectiveness.
Results
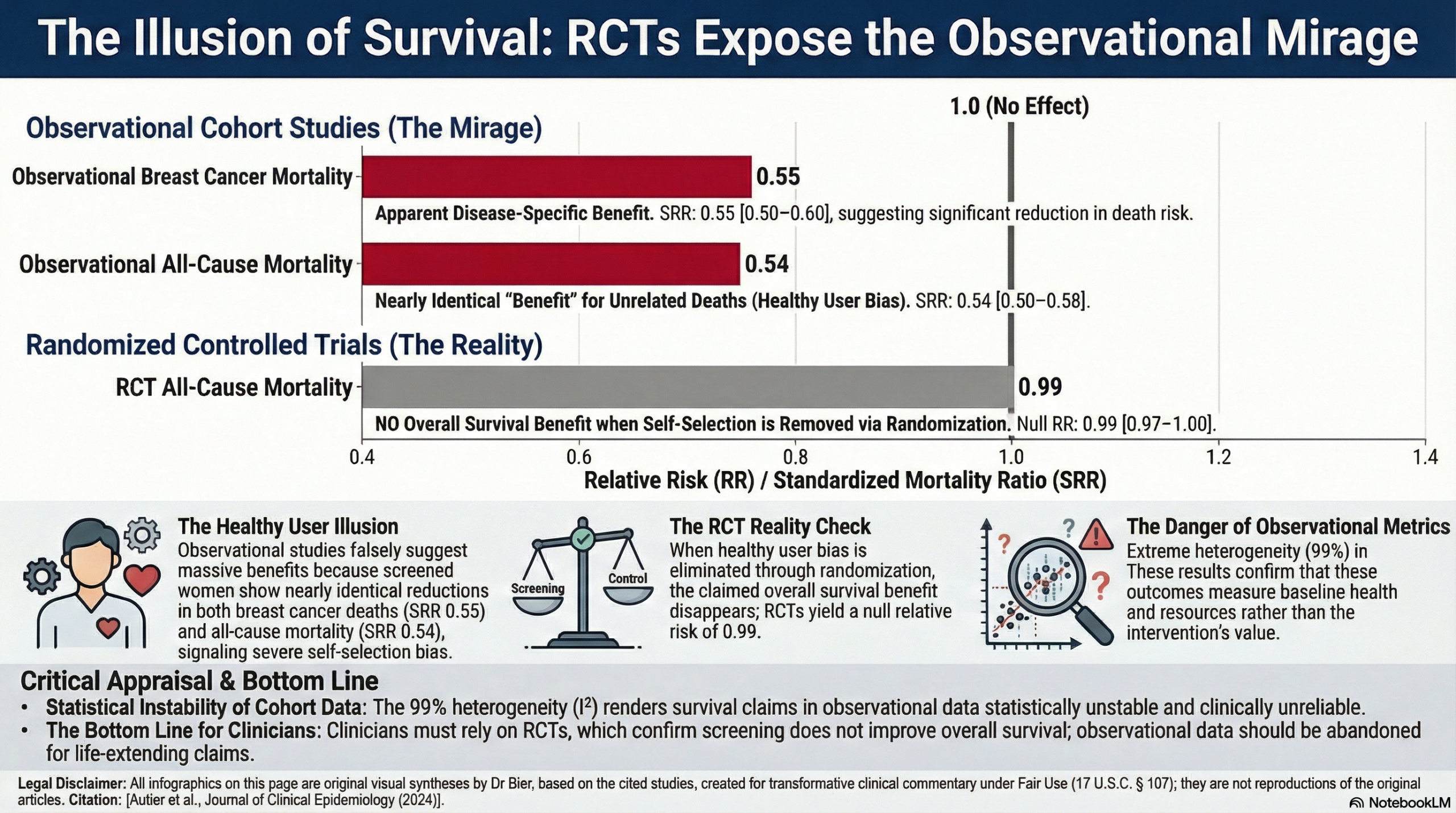
- Summary of Results: In 13 cohort studies, women attending screening had a summary relative risk (SRR) of 0.55 (95% CI: 0.50-0.60) for breast cancer (BC) mortality.
- Off-Target Effects: In 10 cohort studies, the same population of screen-attendees had an SRR of 0.54 (95% CI: 0.50-0.58) for all-cause mortality.
- Direct Comparison: In the four studies that specifically tracked both outcomes in the same cohorts, the risk reduction for BC death (SRR 0.63) was not statistically different from the reduction in all-cause death (SRR 0.54).
- Statistical Definitions: * Relative Risk (RR): A ratio of the probability of an outcome in an exposed group to the probability of an outcome in an unexposed group.
- SRR: A pooled average of the relative risks from multiple studies.
Assertive Critical Appraisal
- Certainty of Evidence (GRADE): The certainty that observational studies provide a reliable estimate of screening benefit is Very Low. The primary reason for downgrading is the extreme risk of confounding/self-selection bias, evidenced by the “protective” effect of mammography against causes of death it cannot possibly influence.
- Heterogeneity: The authors reported an I2 of 99% for all-cause mortality across the studies. Definition: I2 represents the percentage of variation across studies due to real differences rather than chance. An I2 of 99% indicates massive inconsistency, suggesting that the “effect” varies wildly based on the specific characteristics of the population and setting, further pointing to bias rather than a stable biological effect.
- Publication Bias: The authors did not explicitly detail a funnel plot or Egger’s test in the provided text, though they performed a systematic search across major databases (PubMed, Scopus, Web of Science) and checked reference lists.
- Special Consideration for Pooled Results: While the results are highly statistically significant (CIs do not cross 1.0), the clinical significance is undermined by the “Healthy User Bias”. The study correctly notes that in RCTs—where this bias is removed—the reduction in BC death is much smaller (~20%), and there is zero impact on all-cause mortality.
- Reporting Quality (PRISMA): The study mentions a PRISMA diagram in the supplementary materials and describes a clear search strategy and inclusion/exclusion criteria, including a focus on cohort studies published after 2001 to assess the validity of modern correction methods for bias.
Research Objective
PICO Framework:
- Population: Women offered screening mammography.
- Intervention: Attendance at screening mammography.
- Comparison: Non-attendance at screening mammography.
- Outcome: Risk of breast cancer death vs. risk of all-cause or non-breast cancer death.
Study Design
- Design: Systematic review and meta-analysis of observational cohort studies.
- Strategy: Searched for studies published between 2002 and 2022 to evaluate if common statistical “corrections” for healthy user bias actually work.
Setting and Participants
- Studies: 18 cohort studies identified (13 for BC mortality, 10 for all-cause/non-BC mortality).
- Participants: Millions of women across various countries including Canada, UK, Sweden, Australia, and Korea.
Bibliographic Data
- Title: Effect of screening mammography on the risk of breast cancer deaths and of all-cause deaths: a systematic review with meta-analysis of cohort studies
- Authors: Philippe Autier, Karsten Juhl Jørgensen, Michel Smans, Henrik Støvring
- Journal: Journal of Clinical Epidemiology
- Year: 2024
- DOI: 10.1016/j.jclinepi.2024.11.1426
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.