
Comment:
The efficacy of mammography debate is a conflict between the allure of the “early detection saves lives” mantra and the reality that these screenings have never demonstrated a statistically significant improvement in all-cause mortality. The traditional clinical focus on universal mammography ignores the underlying reality that the tradeoff between harms and benefits has been shifting toward harm for decades. To be clear, screening mammograms, where everyone in a population is recommended to do it, is different than a diagnostic mammogram, where there is a particular reason in that individual. I have had numerous patients who detected a lump and did a mammogram to assess it, which is a diagnostic mammogram. Of course, it is also not infrequent that the lump/area of concern turns out to be fine, but a completely separate area is suspicious, which is now a screening mammogram.
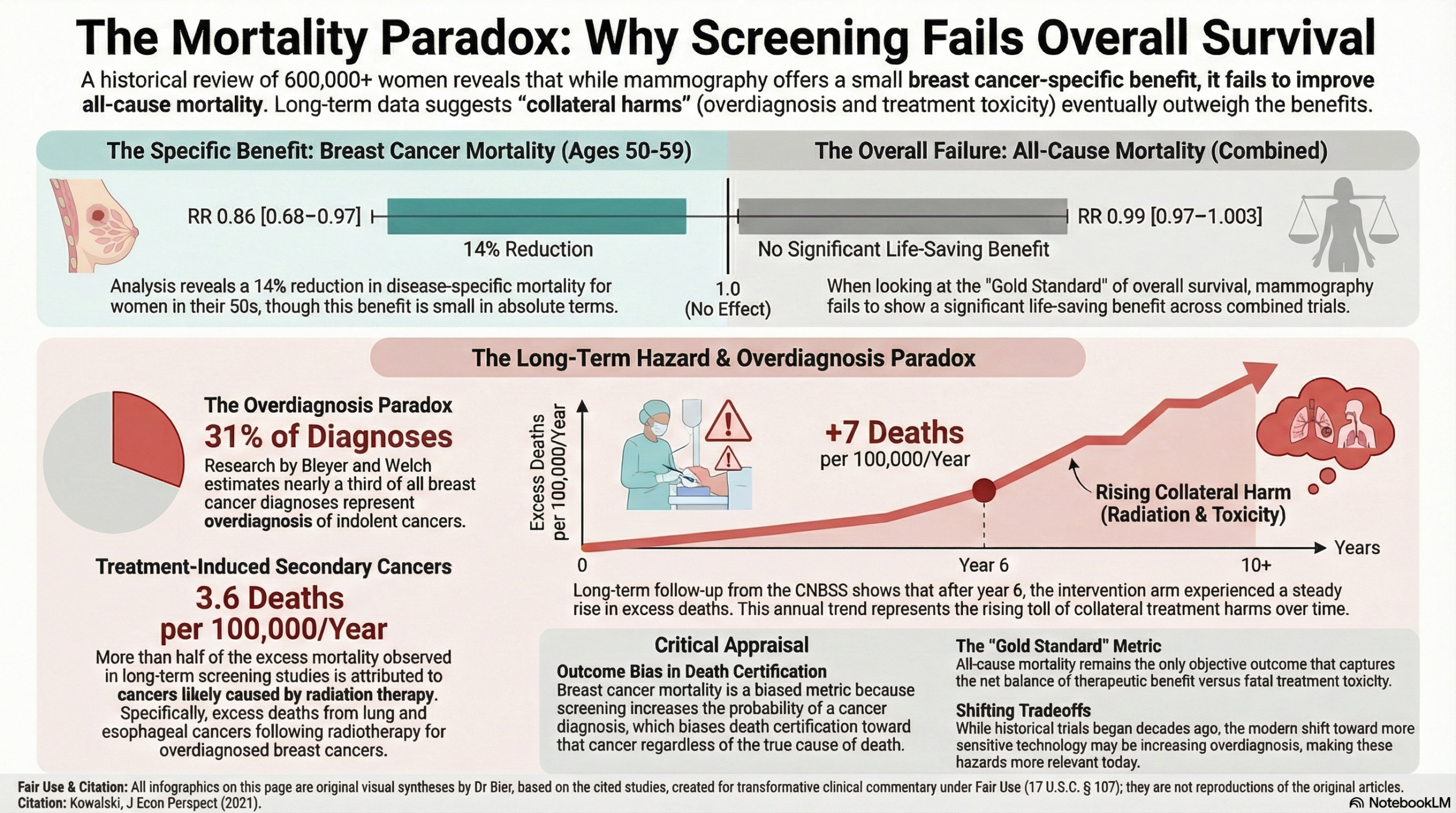
This narrative review deconstructs the historical trajectory of over 600,000 cases to reveal a profound discrepancy: while screening might prevent a handful of disease-specific deaths, it fails the “gold standard” of overall survival. For years, I have cautioned that “breast cancer mortality” is a biased metric; the act of screening artificially increases the probability of a cancer diagnosis, which in turn increases the likelihood that a subsequent death will be coded as such, regardless of the actual cause. We should recognize that the “life-saving” benefits often touted are frequently a mirage, eventually overtaken by the collateral harms of overdiagnosis. While early RCTs suggested a modest reduction in disease-specific deaths, this review demonstrates that these gains have been neutralized by the toxicities of modern treatment for overdiagnosed cancers. This review highlights the “Overdiagnosis Paradox”: screening “skyrockets” the incidence of early-stage cancers without a corresponding decrease in late-stage disease, indicating we are primarily detecting indolent lesions that would never have caused symptoms. In fact, Long-term data from the Canadian National Breast Screening Study (CNBSS) reveals an upward-sloping trend in excess deaths—adding approximately 7 per 100,000 women annually—largely due to radiation-induced cancers from treating these overdiagnosed cases.
The FDA considers Overall Survival (OS) the “gold standard” because it captures the net effect of both therapeutic benefit and fatal toxicity, and on this metric, mammography consistently fails. As difficult as it may be to believe based on decades of habit, the evidence does not support universal screening as a survival-enhancing tool. Overall survival is the only objective outcome for measuring benefit, and mammography screening fails.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
The evidence regarding mammography demonstrates a profound discrepancy between disease-specific benefits and ultimate patient outcomes. While screening may lead to a modest reduction in breast cancer-specific mortality, it has failed to demonstrate a statistically significant improvement in all-cause mortality (Overall Survival) across any age group. In fact, long-term evidence from the Canadian National Breast Screening Study (CNBSS) suggests that the initial life-saving benefits of early detection are eventually overtaken by collateral harms—primarily from overdiagnosis and treatment-related toxicities—leading to a net increase in excess all-cause deaths over a 20-year follow-up.
Key Themes & Evidence Summary
- Scope: This review deconstructs the historical trajectory of eight major randomized controlled trials (RCTs) involving over 600,000 women, tracing the evolution of screening guidelines from universal recommendations (age 40+) to more selective, individualized approaches.
- The Overdiagnosis Paradox: A primary argument is that screening “skyrockets” the incidence of early-stage cancers without a corresponding decrease in late-stage disease. This indicates widespread overdiagnosis—the detection of indolent cancers that would never have caused symptoms or death.
- Disease-Specific vs. Overall Survival:
- Breast Cancer Mortality: Meta-analyses find statistically significant but small absolute reductions: screening 10,000 women aged 50–59 for 10 years prevents only 7.7 breast cancer deaths.
- Overall Survival (All-Cause Mortality): Combined analysis of all trials shows no significant reduction. The FDA considers Overall Survival (OS) the “gold standard” because it captures the net effect of both therapeutic benefit and fatal toxicity.
- Trend in Collateral Harm: Analysis of CNBSS data reveals an upward-sloping trend in excess all-cause mortality, adding approximately 7 excess deaths per 100,000 women each year after enrollment. Over half of this trend is attributed to “collateral harms” like lung and esophageal cancers caused by radiotherapy for overdiagnosed early-stage breast cancers.
Assertive Critical Appraisal
- Evidence Level: This is a Narrative Review (Level 5 Evidence/Expert Opinion), though it is anchored by a high-level synthesis of major RCTs and includes a new empirical analysis of trial data.
- Disease-Specific Bias: The author correctly flags that “breast cancer mortality” is a biased endpoint. Mammography increases the probability of a cancer diagnosis, which in turn increases the likelihood that a subsequent death will be coded as a breast cancer death, even if caused by other factors.
- Overall Survival as the True North: Aligning with FDA guidance, the review emphasizes that OS is the only objective, clinically meaningful endpoint for demonstration of true benefit. Discordant results—where a drug or screening “works” on a surrogate or disease-specific marker but fails on OS—often indicate that treatment-related toxicities outweigh anti-tumor activity.
- Quality Assessment (SANRA Scale):
- Justification & Aims: The review provides a robust justification, addressing the “complicated relationship” between screening and death.
- Literature Search: While it covers the definitive trials in the field (Nelson et al. 2016 meta-analysis), it lacks a pre-specified, transparent search strategy for its own narrative synthesis, which is a common limitation of this study type.
- Scientific Reasoning: The argument is highly logical, particularly the use of 20-year follow-up data to show how the “tradeoff between harms and benefits… has been shifting toward harms over time”.
- Applicability: These findings are critically relevant to general clinical practice, particularly when counseling women in their 40s where the evidence for benefit is weakest and the potential for long-term collateral harm from overdiagnosis is significant.
Research Objective To analyze the evolution of mortality evidence in mammography trials and explore why all-cause mortality may diverge from breast cancer-specific mortality over time.
Bibliographic Data
- Title: Mammograms and Mortality: How Has the Evidence Evolved?
- Authors: Amanda E. Kowalski
- Journal: Journal of Economic Perspectives
- Year: 2021
- DOI: 10.1257/jep.35.2.119
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.