
Comment:
This prospective cohort is the initial study on false-positive mammograms later followed up about a decade later is this study. The data is staggering: six months after receiving a final benign diagnosis, meaning knowing the original finding was false and that they were now ‘normal’, women with false alarms reported negative changes in existential values equal to women who were actually diagnosed with breast cancer.
Although it is simple, or maybe simplistic to assume that the extra stress goes back to normal after finding out all is clear, this study again shows that subjecting a healthy woman to the acute terror of a potentially lethal malignancy fundamentally rewrites her neurological baseline. This study proves the trauma does not evaporate. Three years later, these women still reported greater negative psychosocial consequences across all 12 measured outcomes compared to those with normal screens. And it’s follow-up shows some of that persists a decade after that.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
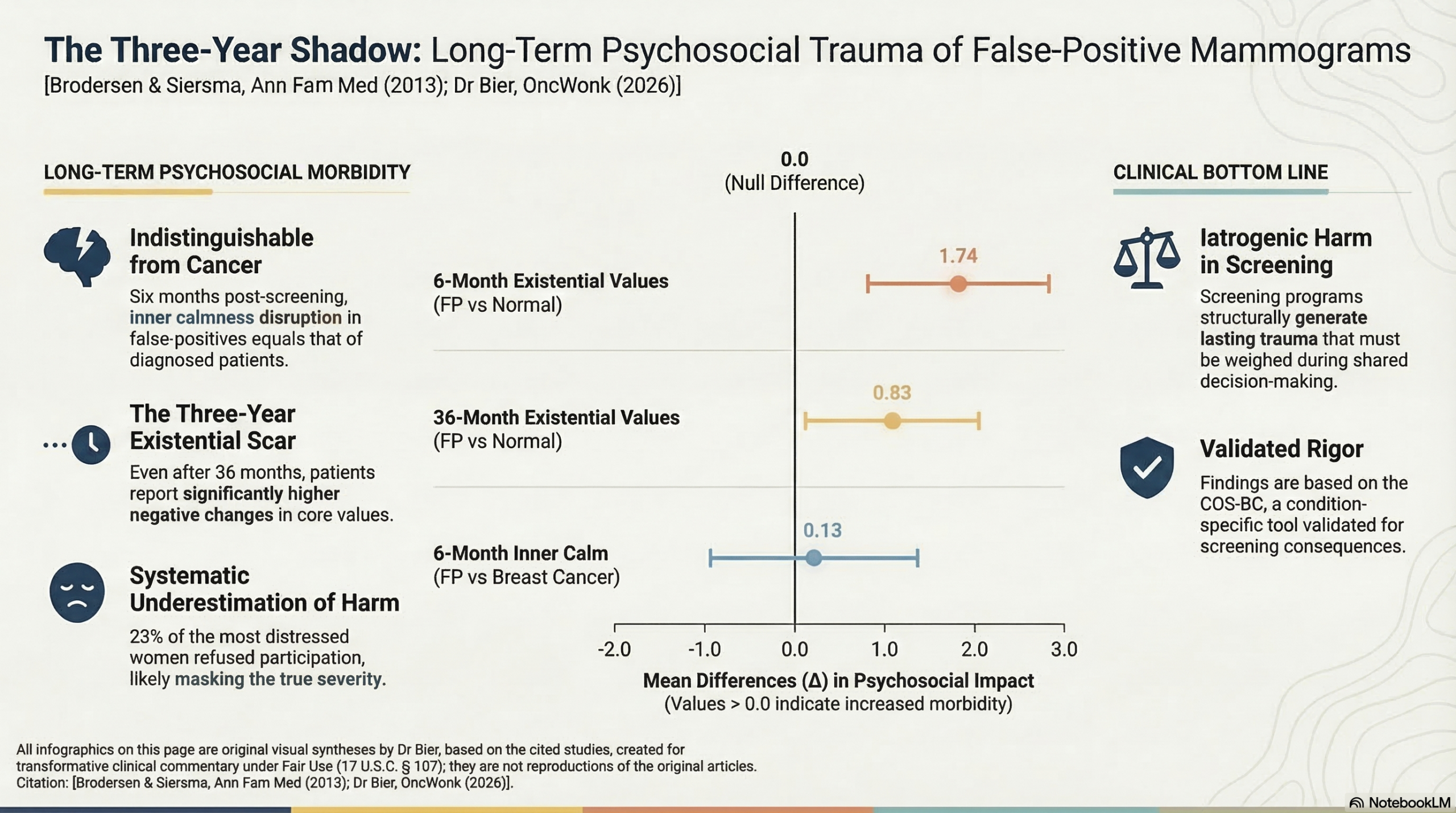
This prospective cohort study demonstrates that a false-positive mammogram is not a transient stressor but carries long-term psychosocial harm that persists for at least three years. While the acute distress of women with false-positives is significantly higher than those with normal results, the most striking finding is that six months after being cleared of cancer, these women reported changes in existential values and inner calmness equivalent to women actually diagnosed with breast cancer. Clinicians should recognize that “all-clear” results after a recall do not immediately or fully resolve the psychological trauma induced by the suspicion of cancer.
Results in Context
- Main Results: Three years after the final diagnosis, women with false-positive results reported greater negative psychosocial consequences compared to women with normal findings across all 12 measured outcomes ($\Delta > 0$ for 12/12 outcomes; $P < .01$ for 4/12).
- Definitions: * $\Delta$ (Mean Difference): Represents the difference in average scores on the COS-BC scale between groups; a positive value indicates higher psychosocial impact in the second group.
- P-value: The probability that the observed difference occurred by chance; the study used a strict threshold of $P < .01$ to minimize false-positive statistical findings.
- Comparison to Breast Cancer Patients: Six months post-diagnosis, the impact on “existential values” (e.g., pessimism about the future) and “inner calmness” was statistically indistinguishable between women with false-positives and those with true breast cancer ($\Delta = 1.15; P = .015$ and $\Delta = 0.13; P = .423$, respectively).
- Participants: The study recruited 454 women with abnormal findings (174 true positives/breast cancer and 272 false positives) and 864 matched women with normal results.
Assertive Critical Appraisal
Limitations & Bias (STROBE Framework)
- Confounding: The authors did not record participants’ family history of breast cancer or prior screening experiences, which are known to influence psychological responses to screening. While they adjusted for age—a proxy for screening experience—unmeasured confounding remains possible.
- Selection Bias: Approximately 23% of women with abnormal findings did not participate, often due to being “too scared” by the initial result. This suggests the study likely underestimated the true negative psychosocial impact, as the most distressed women may have opted out.
- Measurement Bias: Data collection for the “abnormal” group began at the clinic (under high stress), while the “normal” group completed theirs at home. This difference in environment could introduce reporting bias.
Reporting Quality Assessment (STROBE)
The study demonstrates high reporting quality by clearly describing the prospective cohort design and the use of the Consequences of Screening in Breast Cancer (COS-BC) questionnaire, a validated, condition-specific tool. Critically, the authors detail their efforts to address missing data (attrition) using inverse probability weighting, which strengthens the validity of the longitudinal findings.
Applicability
The findings are highly relevant to primary care and radiology. The cumulative risk of a false-positive in the U.S. over 10 screening rounds is 20% to 60%. This study provides a concrete benchmark for the “harm” side of the benefit-harm balance in cancer screening, moving beyond short-term anxiety to documented long-term existential impact.
Research Objective
To measure the psychosocial consequences of false-positive mammography over a three-year period using a condition-specific, validated questionnaire compared to both normal results and a diagnosis of breast cancer.
Study Design
A prospective cohort study with a 3-year follow-up. Participants were assessed at baseline (at the time of abnormal finding/recall), 1, 6, 18, and 36 months.
Setting and Participants
- Setting: Two publicly financed screening programs in Denmark (Copenhagen and Funen) between 2004 and 2005.
- Participants: Women aged 50–69 years invited for biannual screening. The final analyzed cohort included 1,310 women (864 normal, 272 false-positive, 174 breast cancer).
Bibliographic Data
- Title: Long-Term Psychosocial Consequences of False-Positive Screening Mammography
- Authors: John Brodersen, PhD; Volkert Dirk Siersma, PhD
- Journal: Annals of Family Medicine
- Year: 2013
- DOI: 10.1370/afm.1466
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.