
Comment:
This updated meta-analysis shows the failure of “sexual activity”—when broadly defined by intercourse frequency (OR = 1.02)—to provide any credible oncological signal, contrasted against the robust protective effect of mechanical prostatic clearance. The findings are unequivocal: while most sexual behaviors are statistical artifacts, ejaculation frequency demonstrates a statistically significant protective effect (OR = 0.83). The data highlights a specific threshold: men reporting ≥ 21 ejaculations per month demonstrate a 20% reduction in prostate cancer risk, although we don’t have a breakdown according to grade of prostate cancer.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
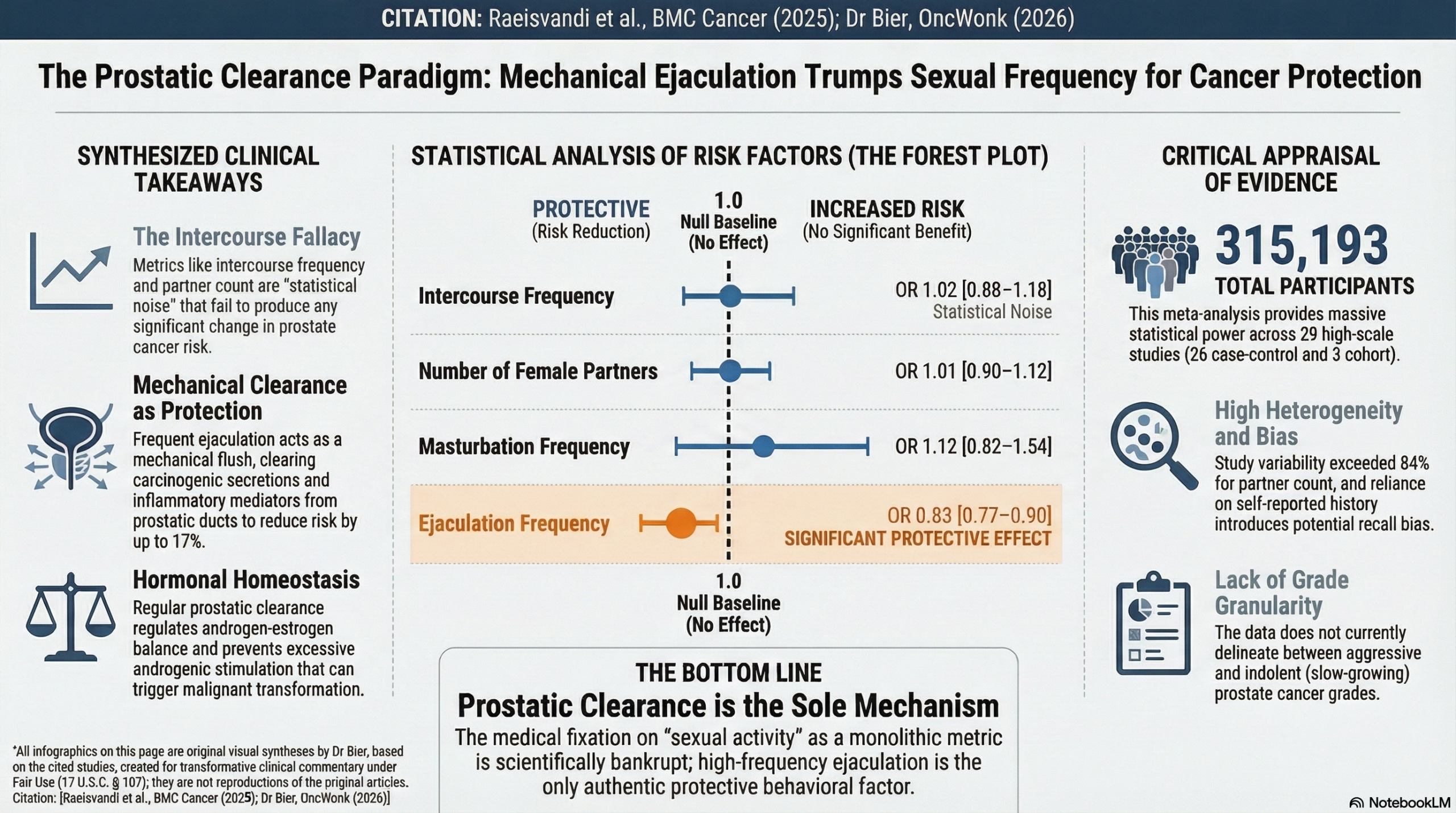
This updated meta-analysis suggests that most sexual behaviors—including frequency of intercourse, number of sexual partners, and age at first intercourse—are not significantly associated with the risk of developing prostate cancer. However, the study identifies a significant protective effect associated with higher ejaculation frequency (OR=0.83; 95% CI: 0.77, 0.90), indicating a 17% reduction in risk for those with higher frequencies. While the findings for ejaculation are supported by moderate certainty, the evidence for other sexual activities remains of low to very low certainty due to high heterogeneity and risk of bias in the primary studies.
Results
- Ejaculation Frequency: Demonstrated a statistically significant protective effect (OR=0.83; 95% CI: 0.77, 0.90). A linear dose-response analysis confirmed that the risk of prostate cancer decreases as the number of ejaculations increases.
- Sexual Intercourse Frequency: Showed a slight, non-significant increase in risk (OR=1.02; 95% CI: 0.88, 1.18). Only the subgroup of \ge1 to <1 times per week showed a significant increase (OR=1.14), which may be a statistical artifact given the lack of a clear dose-response trend.
- Number of Female Sexual Partners: No significant association was found (OR=1.01; 95% CI: 0.90, 1.12).
- Age at First Intercourse: No significant association observed (OR=0.99; 95% CI: 0.90, 1.08), suggesting that the timing of sexual initiation does not materially impact later cancer risk.
- Masturbation Frequency: A positive but non-significant association was reported (OR=1.12; 95% CI: 0.82, 1.54) based on very limited data.
- Prostate Cancer Grade: The meta-analysis analyzed “prostate cancer of any type” that was pathologically confirmed. While it referenced specific studies (e.g., Papa et al. 2017) that investigated aggressive prostate cancer, this meta-analysis did not provide a separate pooled analysis or specific data broken down by Gleason grade or disease severity.
Assertive Critical Appraisal
- Certainty of Evidence (GRADE): The authors applied the GRADE framework and expressed “serious concerns” regarding the evidence for intercourse frequency, partner count, and age at first intercourse due to risk of bias and inconsistency. Only the evidence for ejaculation frequency was rated as “moderate” to “very confident”.
- Heterogeneity: Substantial heterogeneity was observed in several analyses, particularly for the number of female partners (I2=84%) and age at first intercourse (I2=78%). Heterogeneity represents the percentage of variation across studies due to real differences (such as study design or population) rather than chance; these high values suggest the pooled averages for these variables should be interpreted with extreme caution.
- Publication Bias: Assessed via Begg’s and Egger’s tests. Significant publication bias was detected only for the number of female sexual partners (p=0.003), suggesting that smaller, negative studies may be missing from the literature, potentially skewing the results.
- Risk of Bias in Included Studies: Of the 29 included studies, only 17 (58%) were classified as high quality, while 12 were deemed low quality based on the Newcastle-Ottawa Scale.
- Reporting Quality (PRISMA): The study followed PRISMA guidelines and included a clear flow diagram (Fig. 1) detailing the transition from 5,311 identified records to the 29 included studies, ensuring transparency in the selection process.
Research Objective
To update the evidence regarding the association between various sexual activity factors (intercourse frequency, number of partners, age at first intercourse, ejaculation frequency, and masturbation) and the risk of prostate cancer using a dose-response meta-analysis.
Study Design
A systematic review and dose-response meta-analysis of observational studies (case-control and cohort). A random-effects model was used to calculate pooled odds ratios (OR).
Setting and Participants
- Data Sources: PubMed, Web of Science, and Scopus up to October 19, 2025.
- Total Participants: 29 studies involving 315,193 participants.
- Study Types: 26 case-control studies and 3 cohort studies.
Bibliographic Data
- Title: Updated dose-response meta-analysis of sexual activity and prostate cancer risk
- Authors: Abouzar Raeisvandi, Sanaz Omidi, Massoumeh Javaheri, Hanieh Moradi, Jalal Poorolajal
- Journal: BMC Cancer
- Year: 2026 (Published online Dec 2025)
- DOI: https://doi.org/10.1186/s12885-025-15410-3
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.