
Comment:
This is another paper solidifying the serious cost of a common issue with screening mammograms – the high rate of false positives. When comparing healthy women subjected to a false positive against those with normal screens, the recalled cohort faced massive initial spikes in dejection (OR 15.52) and anxiety (OR 11.09). While it is tempting to assume this resolves with a negative follow-up scan or clean biopsy, the data confirms distress levels remain statistically stagnant between 6 and 12 months, leaving these women with roughly triple the odds of chronic anxiety and sleep disruption a year after the false-positive.
As I’ve written in other reviews, subjecting a healthy woman to the terror of a potentially lethal malignancy creates a profound systemic stress response that a simple “all clear” letter does not dispel. The radiographic false alarm leads to a cascade of stress that results in a persistent existential dread.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
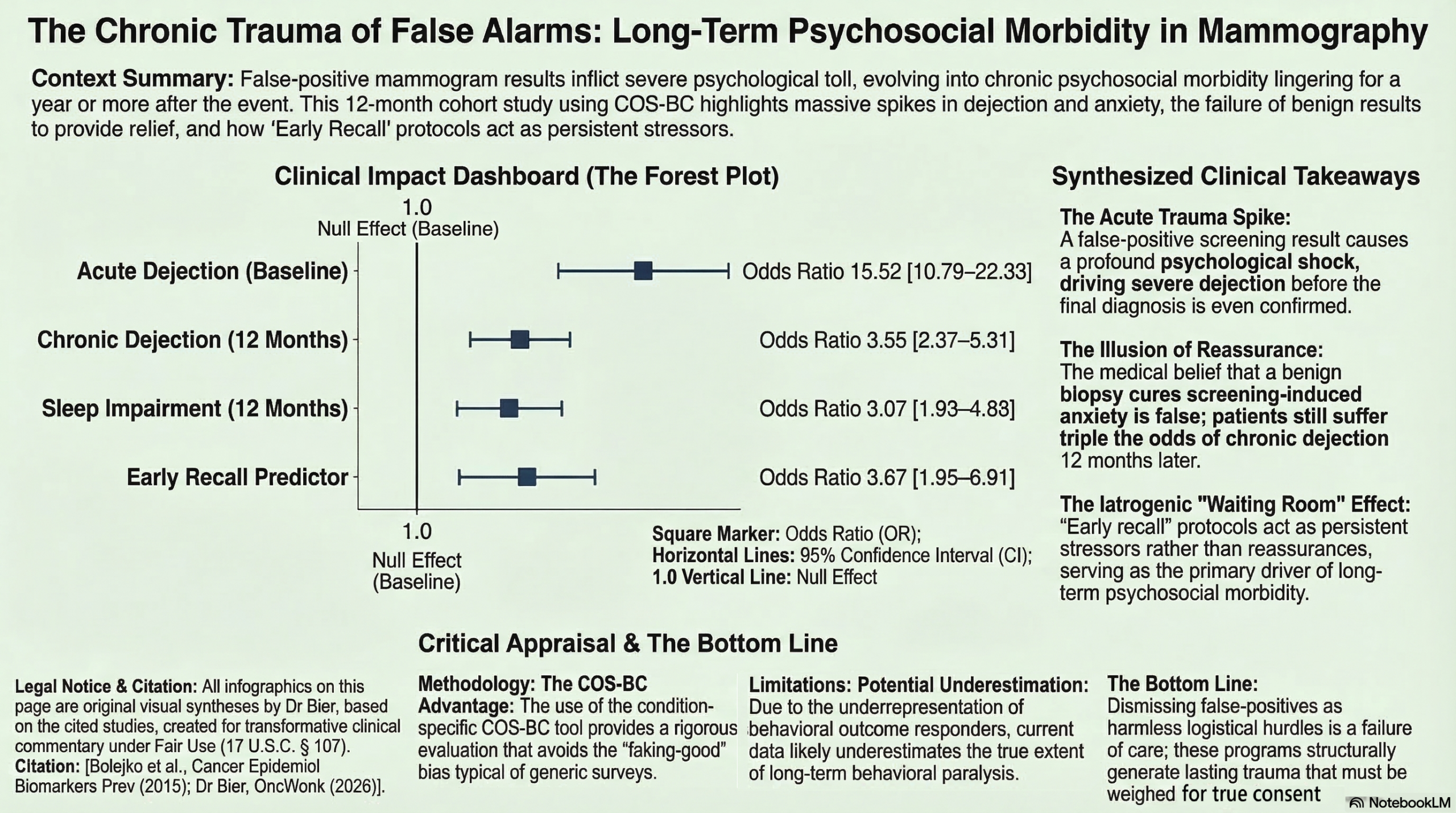
This longitudinal cohort study provides robust evidence that a false-positive mammogram is not a transient stressor; it induces significant psychosocial distress—including dejection, anxiety, and sleep disturbances—that persists for at least one year. While distress levels decline after the initial negative diagnosis, they remain substantially higher than those of women with normal screening results. The strongest predictor of long-term negative impact is early recall (scheduling follow-up imaging in 4–6 months rather than the standard 18–24 months), which likely fosters a “waiting room” effect of prolonged uncertainty. Clinicians should prioritize clear, personalized communication and recognize that foreign-born women or those lacking social support are at higher risk for persistent psychological morbidity.
Results in Context
Main Results
Women experiencing a false-positive result had a significantly higher prevalence of psychosocial consequences across all measured domains (Sense of dejection, Anxiety, Behavioral, Sleep, and Existential values) compared to controls at all time points (P < 0.001).
Magnitude of Effect: At baseline, before receiving a negative diagnosis, the odds of experiencing dejection were more than 15 times higher in the false-positive group than in controls (OR = 15.52; 95% CI, 10.79–22.33).
Long-term Persistence: Distress levels attenuated but did not evaporate. At 6 months, the odds for all consequences were 3.04 to 4.32 times higher than controls; by 12 months, the odds remained significantly elevated at 2.75 to 3.55 times higher.
Predictors of 12-Month Distress:
- Early Recall: This “waiting room” procedure was the most potent driver of chronic distress, with odds 3.05 to 3.67 times higher at one year (down from a 6-month peak OR of 10.31).
- Foreign-Born Status: Associated with a persistent 2.35 to 3.02-fold increase in long-term consequences.
- Lack of Social Support: Remained a stable predictor with an OR of 1.13 to 1.25.
- Clinical Note: While dissatisfaction with information at recall was a significant predictor at 6 months (OR = 2.28–2.56), it failed to reach statistical significance as a predictor of distress at the 12-month mark.
Definitions
- Odds Ratio (OR): A measure of association between an exposure (false-positive result) and an outcome (psychosocial distress). An OR of 15.52 means the odds of dejection were roughly 15.5 times higher in the false-positive group than in the negative-screen group.
- False-Positive: Findings on a screening mammogram leading to additional examinations where the woman is eventually confirmed to be free of breast cancer.
Participants
The study included 399 women with false-positive results (Group I) and 449 age-matched controls with negative results (Group II). Participation rates were 74% for the false-positive group and 56% for the control group.
Assertive Critical Appraisal
Limitations & Bias (STROBE Framework)
- Selection Bias: There was a notably higher non-consent rate among the control group (44%) compared to the false-positive group (26%). While sociodemographic variables were largely balanced, this differential participation could slightly skew the baseline “normal” distress levels.
- Attrition Bias: Women experiencing behavioral consequences at baseline were less likely to complete follow-up. This suggests the study may actually underestimate the true long-term behavioral impact of false-positive results.
- Recall Bias: Baseline data were collected retrospectively (asking women to recall how they felt before the final diagnosis), which may introduce bias, though this was done for ethical reasons to avoid aggravating distress during the diagnostic work-up.
Reporting Quality Assessment (STROBE)
The study demonstrates high reporting quality, explicitly detailing the participant flow, the use of a validated, condition-specific instrument (COS-BC), and a clear description of potential confounders like education, marital status, and country of origin. The authors clearly addressed confounding through multivariate logistic regression models.
Applicability
The findings are highly relevant to population-based screening programs. The identification of “early recall” as a major driver of distress is clinically actionable: clinicians should weigh the low diagnostic yield of early recall against the clear psychological harm it causes. The results also underscore the need for targeted support for foreign-born populations who may face unique communication barriers or cultural attitudes toward cancer.
Research Objective
To investigate the prevalence, longitudinal development, and predictors of psychosocial consequences (dejection, anxiety, behavioral changes, sleep issues, and existential values) following a false-positive breast cancer screening result over a 12-month period.
Study Design
A 1-year longitudinal, age-matched cohort study. Outcomes were measured at three intervals: Baseline (immediately after negative diagnosis), 6 months, and 12 months.
Setting and Participants
- Setting: Three municipalities in southern Sweden, including Malmö, within an established population-based screening program.
- Participants: Swedish-speaking women aged 40–75. Women who felt a lump were excluded to focus strictly on screening-detected findings.
Bibliographic Data
- Title: Prevalence, Long-term Development, and Predictors of Psychosocial Consequences of False-Positive Mammography among Women Attending Population-Based Screening
- Authors: Anetta Bolejko, Peter Hagell, Christine Wann-Hansson, Sophia Zackrisson
- Journal: Cancer Epidemiology, Biomarkers & Prevention
- Year: 2015
- DOI: 10.1158/1055-9965.EPI-15-0060
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.