
Comment:
A true risk-benefit analysis of any intervention should take into account all of the risks, including the psycho-emotional. This cross-sectional study is another that highlights the stark conflict between the conventional narrative of risk-free surveillance and the documented reality of its psychiatric fallout. We know from other studies that I’ve reviewed of the significant risk of overdiagnosis and over treatment What is less acknowledged is the permanent psychological trauma that is induced by a false-positive results, of which there are several strong studies.
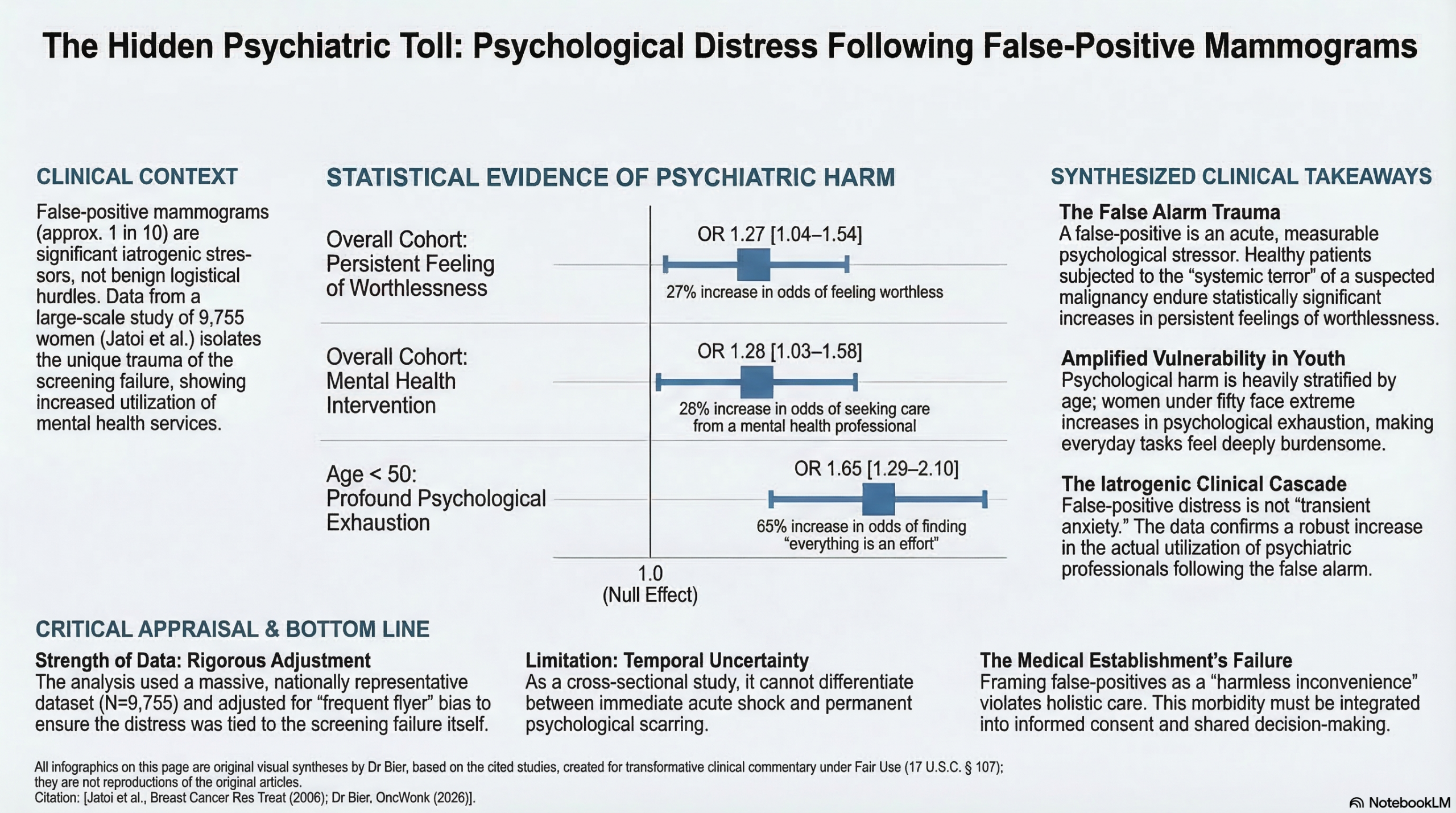
Analyzing 9,755 women, the authors found that the 15% who endured a false positive carried a significantly higher composite distress score (p < 0.0001). Younger women, in particular, were heavily impacted, facing a 27% increased risk of feeling that everything in life was an effort (OR 1.27), while the cohort as a whole saw a 28% increase in mental health professional visits (OR 1.28).
We must acknowledge that subjecting a healthy person to the terror of a lethal malignancy creates a profound systemic stress response. We are actively trading a radiographic false alarm for a cascade of persistent feelings of worthlessness and restlessness. With a life-time risk of a false-positive from mammography screening rising as high as 60% in some studies, pretending that a woman can just can just get over it is a form of gaslighting.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This large-scale observational study suggests a significant and potentially persistent association between false-positive mammograms and increased psychological distress, including symptoms of anxiety and depression. While clinical guidelines emphasize the life-saving benefits of mammography, clinicians should be aware that roughly 1 in 10 screenings result in a false-positive in the U.S., which may lead to measurable increases in sadness, restlessness, and worthlessness, even after cancer is ruled out. Notably, younger women and African-American women may be particularly vulnerable to these psychological sequelae.
Results in Context
- Main Results: After adjusting for numerous confounders, women with a history of false-positive mammograms were significantly more likely to report:
- Feeling sad: OR = 1.18 (95% CI, 1.03–1.35).
- Feeling restless: OR = 1.23 (95% CI, 1.08–1.40).
- Feeling worthless: OR = 1.27 (95% CI, 1.04–1.54).
- Finding everything was an effort: OR = 1.27 (95% CI, 1.10–1.47).
- Seeking mental health care: These women were 28% more likely to have seen a mental health professional in the preceding 12 months (OR = 1.28, 95% CI, 1.03–1.58).
- Definitions: An Odds Ratio (OR) represents the odds of an outcome occurring in an exposed group compared to an unexposed group; an OR of 1.27 indicates a 27% increase in the odds of that symptom.
- Participants: The study analyzed data from 9,755 women who had undergone mammography, of whom 1,450 had experienced a false-positive result.
Assertive Critical Appraisal
- Limitations & Bias (STROBE Framework):
- Confounding: While the authors adjusted for an extensive list of variables (e.g., socioeconomic status, healthcare utilization, and health behaviors), the retrospective nature of the study means unmeasured confounding cannot be entirely excluded.
- Recall Bias: The study relies on self-reported data. Women with existing anxiety or depression might be more likely to remember and report a stressful event like a false-positive mammogram.
- Time Interval: A major limitation is the lack of data on the time elapsed since the false-positive result. It is unclear if the distress observed is acute or represents a long-term “scarring” effect.
- Reporting Quality Assessment (STROBE): The authors provide a robust description of their multivariate models, specifically addressing the risk of “frequent flyer” bias—where women who see doctors more often are both more likely to get screened and more likely to be diagnosed with distress. By adjusting for “bed days” and general practitioner visits, they strengthened the claim that the distress is specifically associated with the false-positive event.
- Applicability: These findings are highly relevant to U.S. primary care and radiology practices, where false-positive rates (10.7%) are higher than in Europe due to different diagnostic thresholds and litigation concerns.
Research Objective
To discern the association between previous false-positive mammograms and persistent psychological distress (anxiety and depression) in a representative sampling of the U.S. population.
Study Design
This was a cross-sectional observational study analyzing data from the 2000 U.S. National Health Interview Survey (NHIS). Psychological distress was measured using the validated K6 questionnaire, a 6-item scale assessing symptoms over the preceding 30 days.
Setting and Participants
- Setting: U.S. household-based survey conducted by the CDC.
- Eligibility: Caucasian and African-American women aged 40–80 with no history of breast cancer.
- Selection: Multistage area probability design with over-sampling of minority groups to ensure representative data.
Bibliographic Data
- Title: Psychological distress in U.S. women who have experienced false-positive mammograms
- Authors: Ismail Jatoi, Kangmin Zhu, Mona Shah, William Lawrence
- Journal: Breast Cancer Research and Treatment
- Year: 2006
- DOI: 10.1007/s10549-006-9236-6
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.