
Comment:
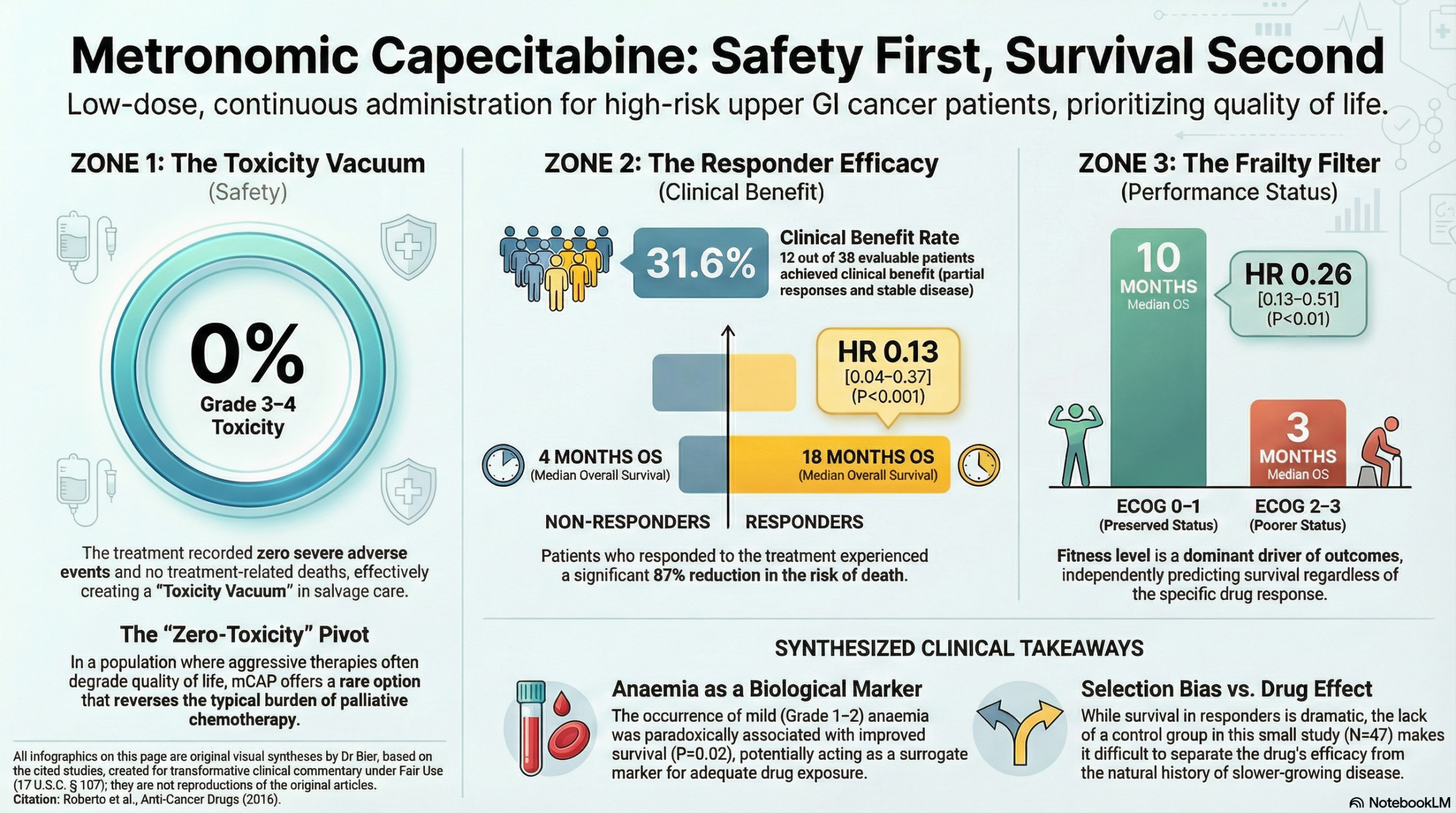
A central issue in palliative oncology is the historical focus on aggressive salvage therapies that frequently lead to negative impacts on QOL rather than measurable survival gains. Metronomic capecitabine reverses this risk-benefit calculation, delivering a median overall survival of 18 months in responders while reporting no treatment-related deaths or severe toxicities. In a population where aggressive options often lead to increased suffering with little benefit, a clinical benefit rate of 31.6% and a remarkable safety profile showing zero Grade 3–4 toxicities, mCAP offers a low risk, higher benefit option.
The tangible significance of this synthesis is the validation of mCAP as a pragmatic salvage option that prioritizes quality of life without sacrificing the potential for disease stabilization. For patients with a preserved performance status (ECOG 0–1), the median overall survival of 10 months demonstrates that meaningful life extension can be achieved without the overwhelming iatrogenic burden of standard chemotherapy.
This is also a place where Naturopathic Medicine shines – improving ECOG scores for both improved QOL and therefore improved outcomes.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This retrospective observational study indicates that low-dose metronomic capecitabine (mCAP) is a safe and moderately active salvage therapy for frail or heavily pretreated patients with advanced upper gastrointestinal (GI) cancers. While it achieved a clinical benefit (CB) in 31.6% of evaluable patients, the benefit was most pronounced in those with a better ECOG performance status (PS 0-1), who experienced a median overall survival of 10 months compared to only 3 months for those with poorer status (PS 2-3). As an observational study, these findings show a strong association between treatment and disease stabilization in a select patient group but cannot definitively prove that mCAP caused the survival benefit due to potential selection bias and the lack of a control group.
Results in Context
- Clinical Benefit Rate: Out of 38 evaluable patients, 12 (31.6%) achieved clinical benefit, which includes one partial response and 11 with stable disease.
- Overall Survival (OS): The median OS for the entire cohort was 5 months.
- Patients responding to treatment (achieving CB) had a significantly longer median OS of 18 months compared to 4 months in non-responders.
- Definition: Overall Survival is the time from the start of treatment until death from any cause; it is considered the “gold standard” for measuring clinical efficacy in oncology.
- Performance Status Impact: A good performance status (ECOG 0-1) was an independent predictor of clinical benefit (Hazard Ratio [HR] = 10.0; P = 0.03) and was associated with significantly longer survival.
- Definition: A Hazard Ratio (HR) represents the relative risk of an event (like death) occurring in one group compared to another. An HR of 0.26 for survival in good PS patients indicates a 74% reduction in the risk of death compared to the poor PS group.
- Safety and Harms: The treatment was remarkably well-tolerated with no Grade 3-4 toxicities or treatment-related deaths reported.
- The most common adverse event was anaemia (14.9%), followed by hypertransaminasemia, hand-foot syndrome, and asthenia (all at 8.5%).
- Interestingly, the occurrence of anaemia was identified as a positive prognostic factor for survival (P = 0.02).
Assertive Critical Appraisal
- Limitations & Bias (STROBE Framework): This is a small, single-center retrospective study (n=47) which inherently carries a high risk of selection bias. The lack of a control group makes it impossible to determine if the observed survival was due to the metronomic capecitabine or simply the natural history of less aggressive disease in certain patients.
- Reporting Quality Assessment (STROBE): The authors provided a detailed breakdown of patient characteristics (Tables 1 & 2) but did not extensively describe efforts to address potential confounding variables beyond multivariate regression. In observational research, unmeasured confounders (e.g., nutritional status, specific prior drug exposures) can significantly skew results.
- Clinical Benefit Definition: The study defined clinical benefit as the sum of complete response, partial response, and stable disease. While useful in salvage settings, “stable disease” can sometimes reflect slow-growing biology rather than drug efficacy, especially in a small sample.
- Applicability: These results are highly relevant to clinicians managing “frail” patients who are ineligible for aggressive multi-drug regimens like FOLFIRINOX or ramucirumab combinations. The oral administration and low toxicity profile make it a practical option for palliative care.
Study Details
- Research Objective: To retrospectively assess the efficacy and safety of low-dose metronomic oral capecitabine as rescue therapy for pretreated or frail patients with recurrent upper gastrointestinal tract cancer.
- Study Design: Retrospective observational cohort study.
- Setting and Participants:
- Location: Sant’Andrea Hospital, Rome, Italy.
- Participants: 47 patients with oesophagogastric (n=25) or pancreatobiliary (n=22) cancers.
- Inclusion: Histological diagnosis, progressive disease at baseline, and inability to tolerate standard chemotherapy due to toxicity concerns or prior failure.
- Intervention: Capecitabine 1500 mg daily, administered continuously without drug-free intervals until progression or toxicity.
Bibliographic Data
- Title: A metronomic schedule as salvage chemotherapy for upper gastrointestinal tract cancer
- Authors: Michela Roberto, Adriana Romiti, Concetta E. Onesti, et al.
- Journal: Anti-Cancer Drugs
- Year: 2016
- DOI: 10.1097/CAD.0000000000000308
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.