
Comment:
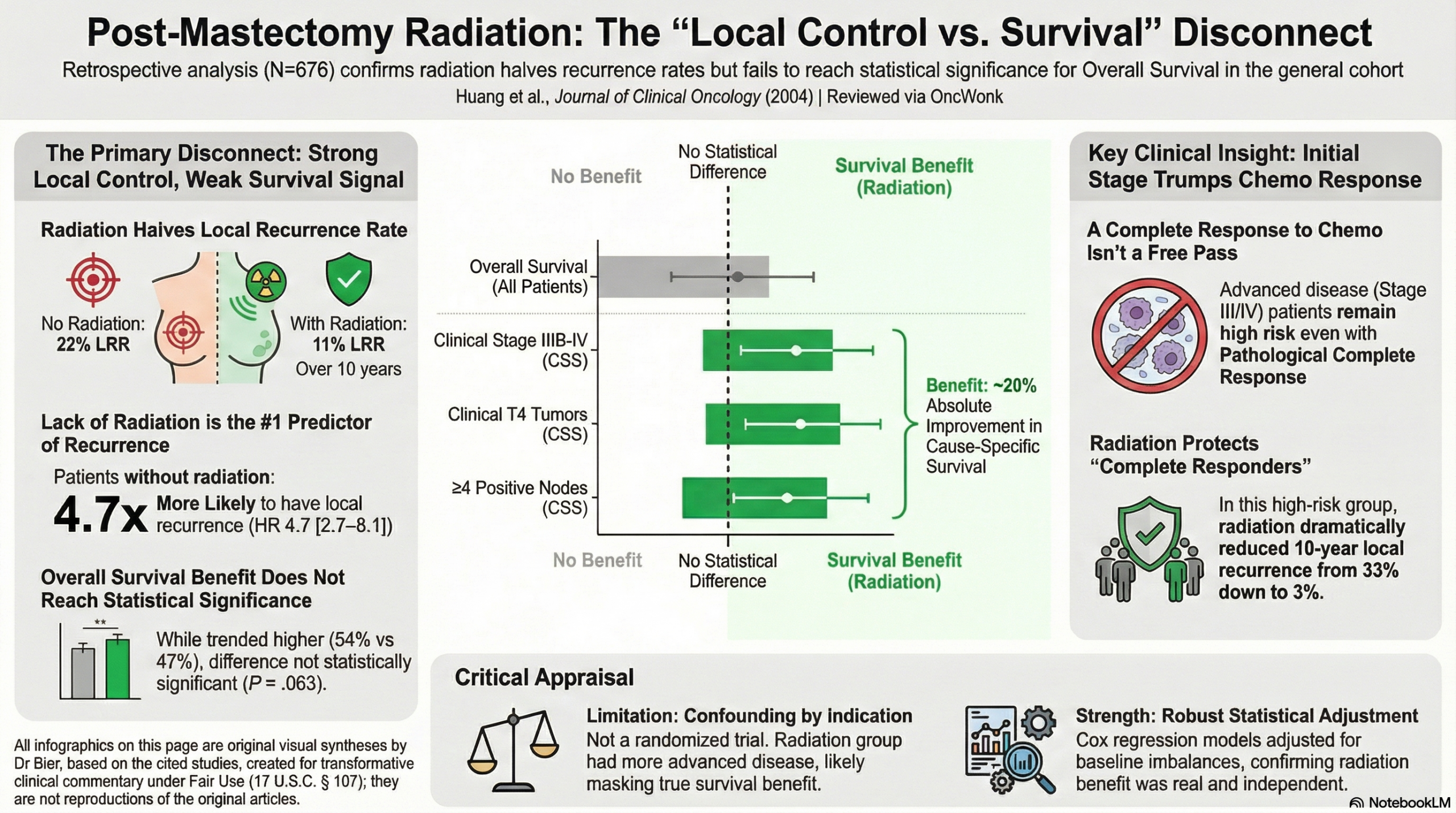
The primary disconnect in this data is the dramatic, nearly five-fold reduction in local-regional recurrence that fails to translate into a statistically significant overall survival benefit for the general cohort. While a 10-year local recurrence rate of 11% compared to 22% is a clear victory for regional management, the P=.063 for overall survival reminds us that we can never assume that local control translates into actual improvement in OS.
Another intriguing aspect is it demonstrates that patients who achieved a pCR still derived a significant local control benefit from radiation if they initially presented with locally advanced disease. The key takeaway is the success of systemic therapy does not erase the risk profile established at the time of diagnosis, so treating as if local cancer cells are present even with pCR is warranted.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This retrospective cohort study demonstrates that postmastectomy radiation (RT) significantly reduces the risk of local-regional recurrence (LRR) in patients treated with neoadjuvant chemotherapy (NCT) and mastectomy. While the study did not find a statistically significant benefit in Overall Survival (OS) for the entire study population (P=.063), it identified a clear Cause-Specific Survival (CSS) and OS advantage for high-risk subgroups, including those with clinical stage IIIB-IV disease, T4 tumors, or four or more positive nodes. Critically, even patients who achieved a pathological complete response (pCR) following NCT still derived a significant local control benefit from RT if they initially presented with advanced disease. Because this is an observational study with significant baseline imbalances—where the irradiated group had more advanced disease—the true benefit of radiation may be even greater than reported.
Results in Context
Main Results: Recurrence and Survival
- Local-Regional Recurrence (LRR): At 10 years, the LRR rate was 11% for the irradiated group versus 22% for the non-irradiated group (P=.0001). On multivariate analysis, the Hazard Ratio (HR) for lack of radiation was 4.7 (95% CI, 2.7 to 8.1; P<.0001), identifying radiation as the most significant variable for local control.
- Overall Survival (OS): The 10-year OS rates were 54% for the RT group and 47% for the no-RT group. This difference did not reach the threshold for statistical significance (P=.063).
- Cause-Specific Survival (CSS): The 10-year CSS (death specifically from breast cancer) for the entire population was 58% with RT versus 55% without (P=.85). However, for high-risk subsets, the benefit was substantial:
- Clinical Stage IIIB-IV: RT improved 10-year CSS from 22% to 44% (P=.002).
- Clinical T4 Tumors: RT improved 10-year CSS from 24% to 45% (P=.007).
- ≥ 4 Positive Nodes: RT improved 10-year CSS from 18% to 44% (P=.005).
Definitions
- Hazard Ratio (HR): A measure of how often a particular event (like recurrence or death) happens in one group compared to another over time. An HR of 4.7 for “lack of radiation” means patients without RT were 4.7 times more likely to experience LRR at any given time.
- Cause-Specific Survival (CSS): A measure of the time from diagnosis or treatment to death only from the disease under study. This is often used to isolate the treatment’s effect on the cancer itself, excluding deaths from other causes like heart disease.
Participants
The study analyzed 676 patients: 542 received postmastectomy RT and 134 did not. All patients were treated on six prospective institutional trials between 1974 and 2000 at M.D. Anderson Cancer Center.
Assertive Critical Appraisal
Limitations & Bias (STROBE Framework)
- Selection Bias: Radiation was not a randomized variable; treatment decisions were made by physicians and patients. This led to a significant “confounding by indication,” where patients with more aggressive disease (higher stage, poorer chemotherapy response) were more likely to receive radiation.
- Historical Cohort: The study spans 26 years (1974–2000), during which systemic therapies (e.g., introduction of taxanes) and radiation techniques evolved.
- Exclusion Bias: To minimize bias, authors excluded 31 patients who recurred very early (within 2 months), which may slightly alter the LRR estimates but improves the comparison of long-term efficacy.
Reporting Quality Assessment (STROBE)
- Confounding: The authors explicitly addressed the baseline imbalances using multivariate Cox regression analysis. By adjusting for these factors, they confirmed that the lack of radiation remained an independent and powerful predictor of both LRR and worse CSS.
- Data Completeness: The study provided clear 10-year actuarial rates and hazard ratios with confidence intervals for both the total population and relevant clinical subgroups.
Applicability
The findings are highly relevant for modern oncology, specifically confirming that the pathological response to neoadjuvant chemotherapy should not be the sole factor in deciding on postmastectomy RT. The study highlights that clinical stage at presentation remains a primary driver of recurrence risk.
Research Objective
To evaluate the efficacy of postmastectomy radiation in patients treated with neoadjuvant chemotherapy and mastectomy, specifically identifying which clinical and pathological subsets benefit in terms of local control and survival.
Study Design
Retrospective analysis of data from six consecutive prospective institutional clinical trials.
Setting and Participants
- Setting: Single institution (The University of Texas M.D. Anderson Cancer Center).
- Inclusion: Patients with nonmetastatic, noninflammatory breast cancer treated with doxorubicin-based NCT and mastectomy.
- Stage: Patients ranged from Stage I to Stage IV (ipsilateral supraclavicular node involvement).
Bibliographic Data
- Title: Postmastectomy Radiation Improves Local-Regional Control and Survival for Selected Patients With Locally Advanced Breast Cancer Treated With Neoadjuvant Chemotherapy and Mastectomy
- Authors: Huang EH, Tucker SL, Strom EA, et al.
- Journal: Journal of Clinical Oncology
- Year: 2004
- DOI: 10.1200/JCO.2004.11.129
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.