
Comment:
While the appeal of ‘radiation-free’ screening is undeniable, the evidence presented in this review should give anyone recommending thermography pause. The extreme variability in diagnostic accuracy—with sensitivity swinging wildly from 25% to 97%—makes these tools clinically unpredictable. Crucially, the complete absence of data on asymptomatic women means we are effectively flying blind if we apply these technologies to healthy populations. Until we have high-quality evidence showing a mortality benefit, relying on thermography or EIS as a substitute for standard mammography offers patients a false sense of security.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
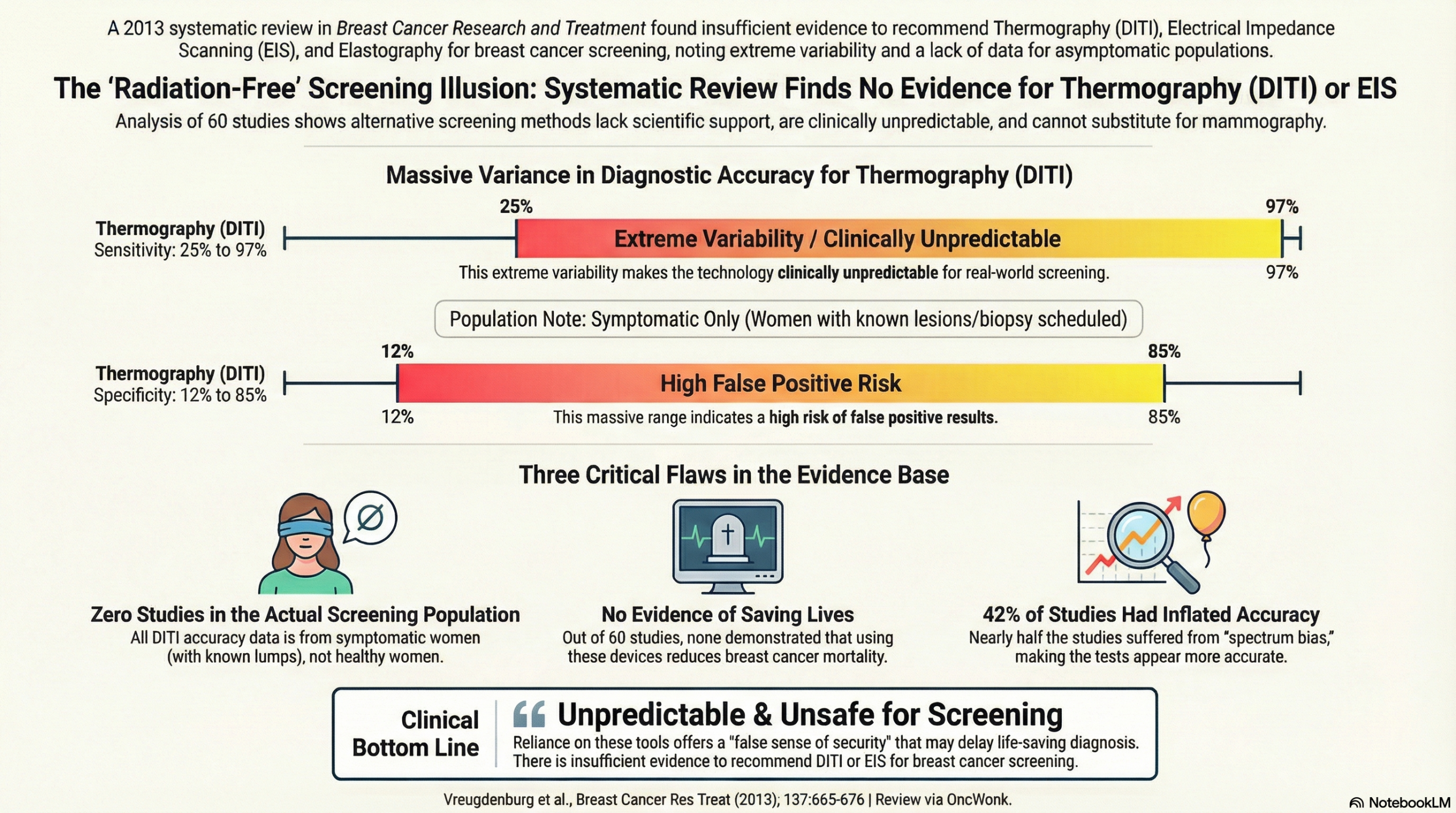
This systematic review concludes that there is insufficient evidence to recommend Digital Infrared Thermal Imaging (DITI), Electrical Impedance Scanning (EIS), or elastography for breast cancer screening. Regarding thermography (DITI) specifically, the review found no studies evaluating its effectiveness in reducing breast cancer mortality and noted that diagnostic accuracy varied wildly across studies. Furthermore, because the available data is derived almost exclusively from symptomatic women (those already suspected of having cancer), these technologies cannot be considered safe or effective for screening healthy, asymptomatic populations at this time.
Results
- Lack of Screening Evidence: The review identified that out of 60 included studies, zero effectiveness studies were found that showed a reduction in mortality attributable to imaging with these devices. For DITI, no studies investigated its use for detecting breast cancer in an asymptomatic (screening) population.
- Thermography (DITI) Accuracy: The review analyzed eight DITI studies. The diagnostic accuracy was highly inconsistent:
- Sensitivity ranged from 25% to 97% (median 82%).
- Specificity ranged from 12% to 85% (median 55%).
- Comparison to Other Modalities: Similar variability was observed for EIS and Ultrasound Elastography (USE). EIS sensitivity ranged from 26% to 98%, and USE sensitivity ranged from 35% to 100%.
- Conclusion on Screening: Due to the absence of data on asymptomatic women and the high heterogeneity in symptomatic populations, the authors state these devices should not be adopted for screening.
Assertive Critical Appraisal
- Certainty of Evidence (High Heterogeneity): The review quantitative assessment revealed significant heterogeneity ($I^2$) across all device classes. For DITI specifically, estimates were so variable that the authors deemed it inappropriate to calculate a pooled estimate of diagnostic accuracy. This extreme variation suggests that the “accuracy” of thermography is highly dependent on the specific device and method used, rather than being a robust clinical standard.
- Risk of Bias in Included Studies: The quality of the primary evidence was generally poor.
- Selection Bias: 63.3% of studies demonstrated selection bias, often due to non-consecutive enrollment, which can inflate diagnostic accuracy estimates.
- Spectrum Bias: 41.7% of studies suffered from spectrum bias, meaning they selectively included patients with advanced disease, making the test appear more accurate than it would be in a real-world setting.
- Blinding: Blinding of the index test (thermography) to the reference standard was reported in only 41.7% of studies. If the interpreter knows the patient has cancer, they are more likely to read the thermogram as “positive,” introducing review bias.
- Publication Bias: The authors assessed for publication bias using Deeks’ funnel plot and found no evidence of significant asymmetry for DITI ($p=0.77$).
- Reporting Quality (PRISMA): The review follows PRISMA guidelines, utilizing a flow diagram and standardized data extraction. However, the conclusions are limited by the low quality of the available primary literature.
Research Objective
To systematically identify and evaluate the evidence of safety, effectiveness, and diagnostic accuracy for three emerging technologies—DITI, EIS, and elastography—promoted for breast cancer screening and diagnosis.
Study Design
- Methodology: A systematic search of seven biomedical databases (including PubMed, EMBASE, and Cochrane) was conducted through March 2011.
- Inclusion Criteria: Studies were eligible if they investigated the use of the relevant index test for detecting breast lesions in humans and compared it to a valid reference test (e.g., biopsy).
- Exclusion: Studies published before 1980 were excluded due to changes in thermal imaging technology.
Setting and Participants
- Total Included: 60 studies met the inclusion criteria.
- DITI Specifics: 8 studies investigated Digital Infrared Thermal Imaging.
- Population: The vast majority of studies involved symptomatic populations (women already scheduled for biopsy or with identified lesions) rather than screening populations.
Bibliographic Data
- Authors: Vreugdenburg TD, Willis CD, Mundy L, Hiller JE.
- Journal: Breast Cancer Research and Treatment.
- Year: 2013.
- DOI: 10.1007/s10549-012-2393-x
Original Article:
Full text: here
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.