
Comment:
Although the concept of thermograph sounds great, the results are not. A fundamental conflict exists between the “health halo” surrounding digital thermography and the reality of the outcomes. Proponents argue that DITI can identify early metabolic shifts, yet the data confirms that it fails at the most basic requirement of a screening tool: identification of the target pathology. With a 75% false-negative rate, thermography is more likely to miss a cancer than to find it, a reality that makes it a liability rather than a supportive diagnostic layer as it gives the patient a false sense of security.
The clinical utility of this study is the confirmation that we cannot substitute “digital” upgrades for biological validity. The fact that standard modalities like ultrasound and mammography outperformed DITI by over 60 percentage points in sensitivity proves that the technology is not ready for clinical deployment.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
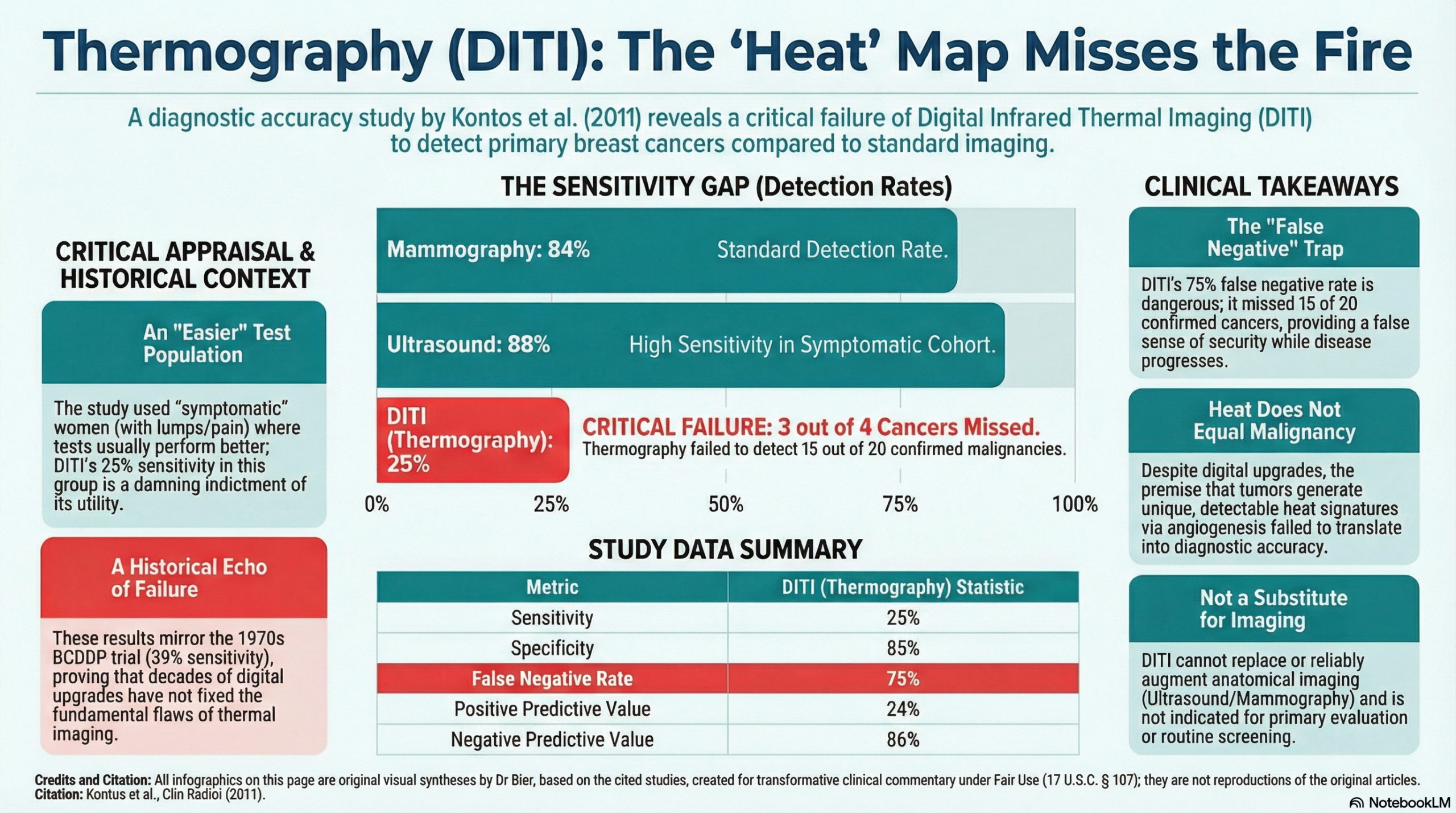
This diagnostic accuracy study provides strong evidence that Digital Infrared Thermal Imaging (DITI) is insufficient for the primary evaluation or screening of breast cancer. The study demonstrated a critically low sensitivity of 25%, meaning the technology missed the vast majority of confirmed malignancies in this cohort. Consequently, the authors conclude that DITI should not be used as a substitute for standard screening methods like mammography or ultrasound.
Results in Context
Diagnostic Accuracy Metrics
The primary aim of the study was to compare DITI against the gold standard of histology (for malignancy) or standard imaging/histology (for benign lesions).
- Sensitivity (Detection Rate): 25%.
- Context: This is the ability of the test to correctly identify patients with the disease. A 25% sensitivity indicates that DITI failed to detect 75% of the cancers present.
- Specificity: 85%.
- Context: This is the ability of the test to correctly identify patients without the disease.
- False Negatives (Missed Cancers): There were 15 false-negative results out of 20 confirmed cancer cases. This is the most clinically dangerous metric, as these patients had cancer that the thermal imaging categorized as normal or benign.
- True Positives: Only 5 cancers were correctly identified by DITI.
Comparison to Standard of Care
The study compared DITI performance to ultrasound and mammography within the same patient group, highlighting a massive disparity in efficacy.
|
Modality |
Sensitivity |
Specificity |
Negative Predictive Value |
|
DITI (Thermography) |
25% |
85% |
86% |
|
Ultrasound |
88% |
91% |
95% |
|
Mammography |
84% |
97% |
96% |
Assertive Critical Appraisal
- Risk of Bias (Sensitivity Analysis): The study utilized a “symptomatic” population (women already presenting with breast complaints) rather than a general screening population. In diagnostic accuracy studies, utilizing a symptomatic population typically increases the pre-test probability of disease and often inflates sensitivity. The fact that DITI achieved only 25% sensitivity even in this “enriched” population is a damning indictment of the technology’s ability to detect tumors.
- Reporting Quality (STARD/QUADAS): The authors transparently reported the raw confusion matrix (90 true-negatives, 16 false-positives, 15 false-negatives, and 5 true-positives). This transparency allows for independent verification of their calculations and confirms the high rate of missed diagnoses.
- Limitations of Technology: The authors note that while DITI is non-invasive and painless, the high number of false positives (16 cases) would lead to unnecessary invasive assessments, and the high number of false negatives (15 cases) provides false reassurance to women with cancer.
- Historical Context: The authors appropriately contextualize their findings with historical data, noting that even older thermography studies from the 1970s (BCDDP) showed poor sensitivity (39%), suggesting that despite “digital” upgrades, the fundamental physiological basis for the test (heat emission) remains a poor discriminator for malignancy.
Research Objective
To determine the sensitivity and specificity of digital infrared thermal imaging (DITI) in women undergoing surgical excision or core biopsy of breast lesions.
Study Design
A diagnostic accuracy study comparing DITI results (classified as T1-T5) with final diagnosis based on histology or conventional imaging.Setting and Participants
- Setting: A one-stop diagnostic breast clinic in the UK.
- Participants: 63 symptomatic patients (126 breasts examined).
- Disease Prevalence: 20 confirmed cancerous lesions were diagnosed in this cohort.
Bibliographic Data
- Title: Digital infrared thermal imaging (DITI) of breast lesions: sensitivity and specificity of detection of primary breast cancers
- Authors: Kontos M, Wilson R, Fentiman I.
- Journal: Clinical Radiology
- Year: 2011
- DOI: 10.1016/j.crad.2011.01.009
Original Article:
Full text: here
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.