
Comment:
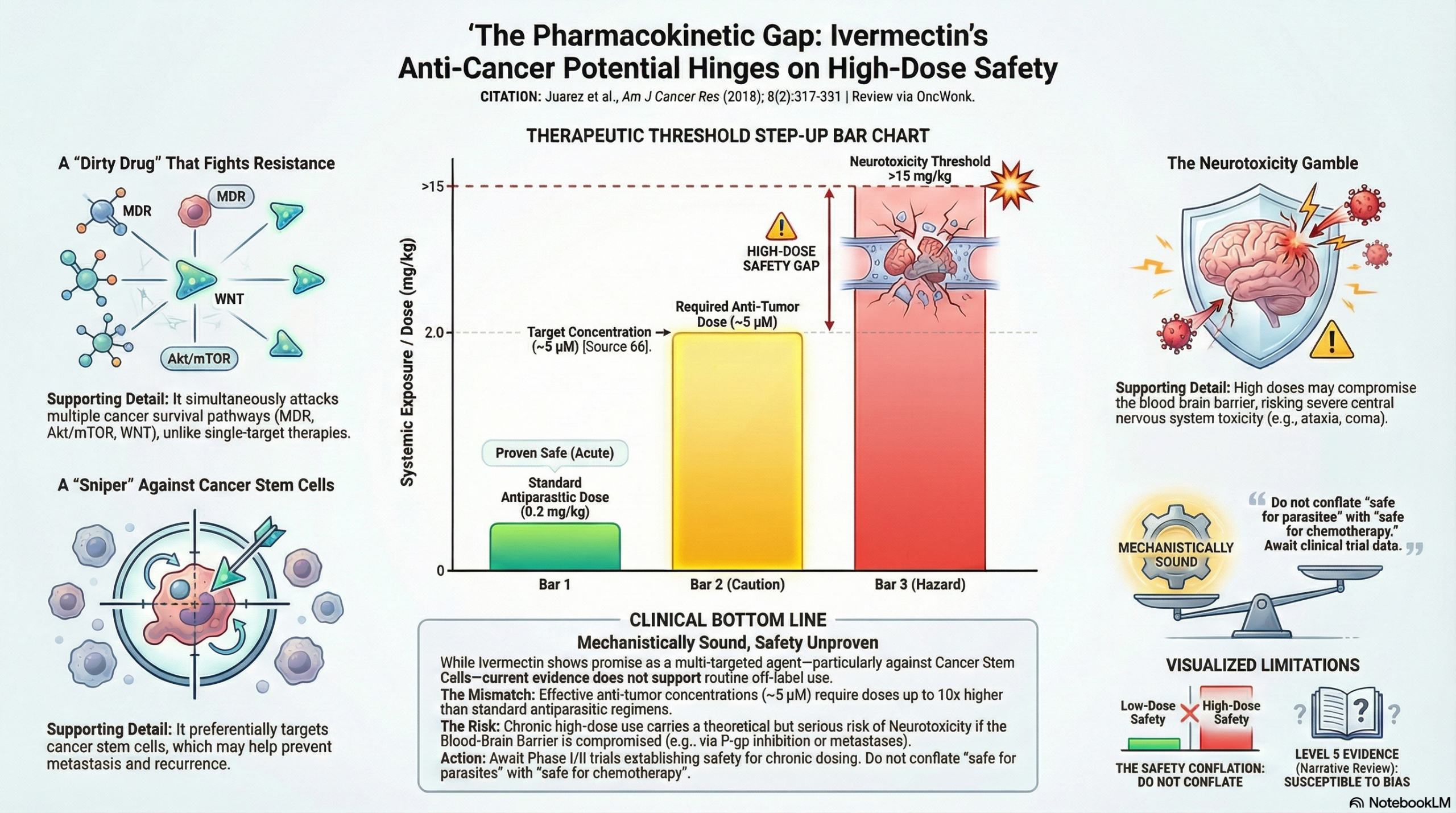
While the mechanism of repurposing ivermectin is mechanistically sound, we must be careful not to conflate “safe for occasional parasitic use” with “safe for chronic oncologic use.” The authors rely on a safety profile established at low, intermittent doses (150–200 mcg/kg). However, achieving the antitumor concentrations cited here likely requires sustained dosing up to 10x higher. My primary concern remains the potential for neurotoxicity; if we are relying on ivermectin to inhibit P-glycoprotein in tumors, we run a theoretical but serious risk of compromising the blood-brain barrier and increasing CNS toxicity in our patients.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This narrative review argues that ivermectin, a widely used antiparasitic, shows significant potential for drug repurposing in oncology due to its multi-targeted mechanism (including MDR inhibition, WNT-TCF pathway modulation, and epigenetic regulation). Regarding safety, the authors contend that ivermectin has a wide therapeutic window and that the concentrations required for antitumor activity are clinically achievable. However, caution is warranted regarding chronic use: the safety profile described relies heavily on low-dose, intermittent antiparasitic regimens, whereas effective cancer therapy would likely require higher, sustained dosing where the risk of neurotoxicity and blood-brain barrier penetration is less well-characterized in humans.
Key Themes & Evidence Summary: Potential Risks of Chronic Use
- Established Safety Profile vs. Cancer Dosing
- Standard Dosing: The authors emphasize that ivermectin has been used safely by billions of people. However, standard antiparasitic doses are low and infrequent (typically 150–200 mcg/kg, occasionally up to 400 mcg/kg).
- Cancer Dosing: To achieve the antitumor concentrations observed in vitro (median ~5microM), significantly higher doses are required. The authors cite pharmacokinetic data suggesting doses up to 2 mg/kg (approx. 10x the standard dose) are necessary to reach these systemic exposure levels (~5.2microM/h).
- Chronic Tolerance: Evidence for high-dose chronic use is limited. The review highlights a single clinical trial for spinal damage where 1.6 mg/kg was administered subcutaneously twice a week for 12 weeks, which was reportedly tolerated.
- Mechanism of Toxicity (Neurotoxicity)
- Blood-Brain Barrier (BBB) Reliance: In mammals, ivermectin toxicity is generally low because the drug is kept out of the central nervous system (CNS) by the P-glycoprotein pump (MDR protein) at the blood-brain barrier.
- Risk Factors: Toxicity increases significantly if P-glycoprotein function is impaired or overwhelmed. This is illustrated by Collie dogs with genetic MDR defects who suffer severe neurotoxicity.
- Clinical Relevance: If ivermectin is used to inhibit P-glycoprotein in cancer cells (to reverse multidrug resistance), there is a theoretical risk that it may also compromise the BBB’s protective function, increasing its own CNS toxicity or that of co-administered chemotherapy agents.
- Symptoms of Overdose and Toxicity
- While therapeutic doses cause few side effects (mostly inflammatory reactions to dying parasites), overdose symptoms indicate neurotoxicity.
- Documented signs of intoxication include ataxia, tremors, mydriasis, motor incoordination, respiratory failure, hypotension, and coma.
- The review notes a case series of poisoning where severe symptoms (coma, aspiration) occurred after mean ingestions of ~15 mg/kg, and one death (multi-organ failure) was reported.
Assertive Critical Appraisal
Evidence Level: Narrative Review (Level 5 Evidence). This is a descriptive overview of existing literature, not a systematic review.
Quality Assessment (SANRA Scale Audit):
- Literature Search (Flagged): The authors do not describe a specific search strategy, inclusion/exclusion criteria, or the time frame of the literature searched. This susceptibility to selection bias allows the authors to present a highly optimistic view of the drug’s safety while potentially excluding studies that might highlight chronic toxicity risks.
- Scientific Reasoning (The “Safety” Gap): The review relies on a logical leap regarding safety. It conflates the safety of annual, low-dose antiparasitic treatment with the safety of high-dose, continuous anticancer treatment.
- The authors state that antitumor activity is achieved at concentrations “clinically reachable”. While technically true that these levels can be reached in plasma, the review does not adequately address the accumulation of toxicity during the sustained daily or weekly dosing required to suppress tumor growth, nor does it fully address the potential for neurotoxicity in cancer patients who may have compromised blood-brain barriers due to metastases or prior radiation.
- Data Presentation: The review provides clear tables comparing in vitro inhibitory concentrations (IC50) with human pharmacokinetic data, which is helpful for benchmarking. However, the lack of human safety data specifically for chronic, high-dose regimens remains a significant evidence gap.
Research Objective
The objective of this review is to summarize in vitro and in vivo evidence demonstrating ivermectin’s antitumor effects and to support its repositioning as a cancer drug based on its safety profile and multi-targeted mechanisms.
Bibliographic Data
- Title: The multitargeted drug ivermectin: from an antiparasitic agent to a repositioned cancer drug
- Authors: Juarez M, Schcolnik-Cabrera A, Dueñas-Gonzalez A
- Journal: Am J Cancer Res
- Year: 2018
- DOI: Not available
Original Article:
Full text: PubMed Central
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.