
Comment:
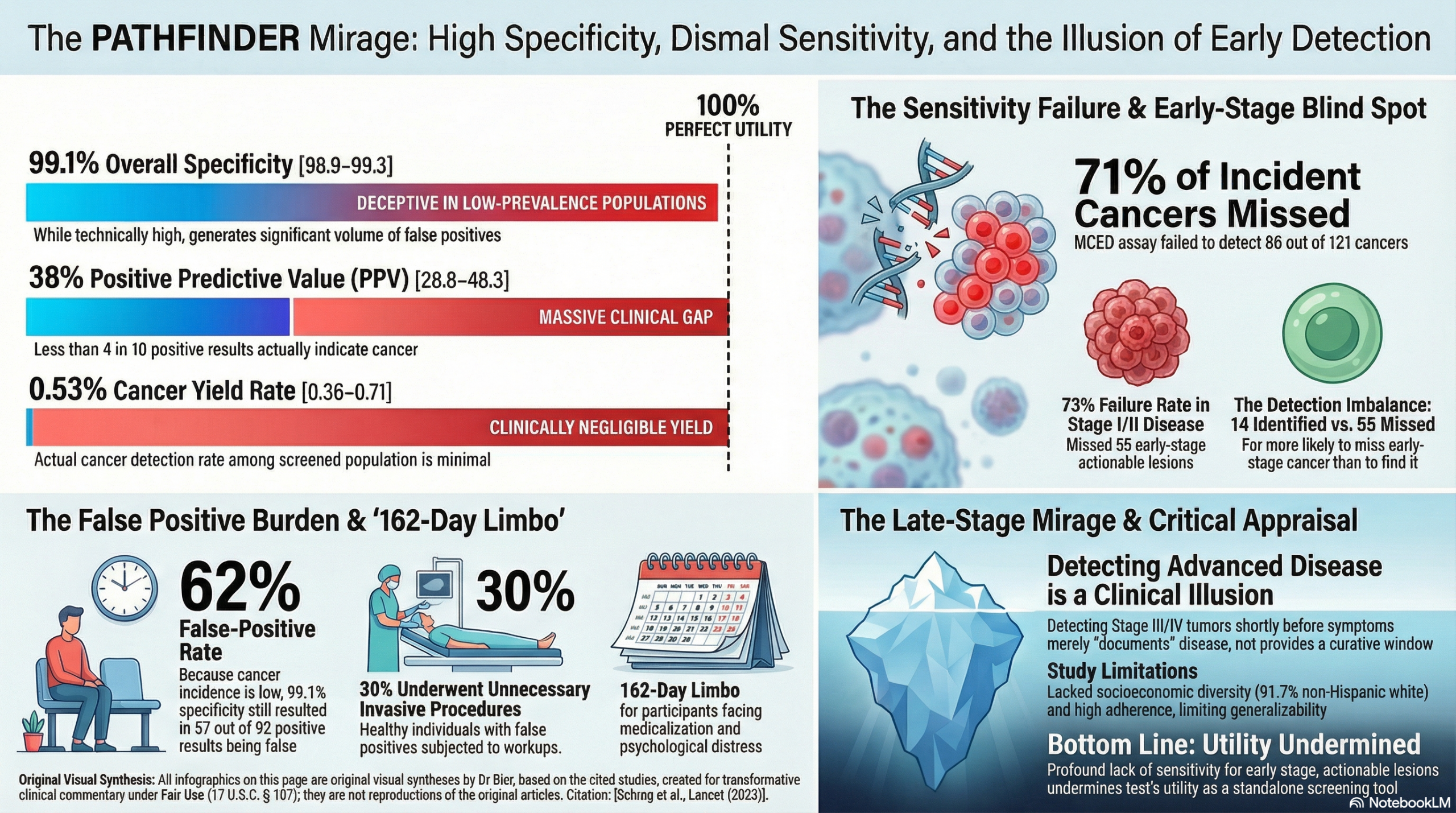
Although I am strong proponent of tests that don’t expose the patient to radiation or unnecessary contrast chemical, there are other types of risks. This study shows that this blood test fundamentally fails to detect early-stage disease, missing 86 out of the 121 cancers (71%) that surfaced during the 12-month study period. More alarmingly, among the new cancers the test failed to detect, a staggering 73% (55 out of 75) were early-stage (Stage I or II). Conversely, the test successfully identified only 14 early-stage lesions. We should recognize that this tool misses the early-stage lesions where intervention matters most, while taxing the healthy with unnecessary medicalization.
While the assay demonstrates higher sensitivity for advanced, later-stage malignancies, this is likely not clinically meaningful. A late-stage tumor sheds more DNA but is also on the verge of producing clinical symptoms that would routinely trigger standard structural imaging. Detecting a Stage III or IV cancer a short time before it becomes clinically obvious is unlikely to alter the survival trajectory; it merely documents the disease. I await later iterations that are more sensitive, but at this point the test misses the early-stage lesions where intervention has a much greater chance to actually matter.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This prospective cohort study demonstrates that multi-cancer early detection (MCED) blood testing is feasible in clinical practice and has high overall specificity, meaning it produces very few false positives relative to the total number of healthy people tested. However, the test missed a substantial number of cancers, particularly those in early stages, highlighting that while the technology is promising, its sensitivity limits its current effectiveness as a standalone early detection tool.
Results in Context
- Main Results: A cancer signal was detected in 1.4% (92 of 6621) of participants who had analyzable blood test results. Diagnostic evaluation confirmed cancer in 35 of these individuals, classifying them as true positives. No cancer was found in the remaining 57 individuals, classifying them as false positives. The blood test yielded an overall specificity of 99.1%.
- Participants: The study enrolled 6662 participants. There were 6621 participants who ultimately had analyzable MCED results.
Understanding the Accuracy Metrics: A Guide for the Clinician
The data provides crucial insights into how well this test performs, particularly regarding false positives and false negatives across different stages of cancer.
- Specificity and False Positives: Specificity is the test’s ability to correctly identify patients who do not have cancer. The study reported a high overall specificity of 99.1%. This means that out of all the truly healthy people tested, 99.1% correctly received a negative result. The remaining 0.9% received a false positive. A false positive means the blood test indicated a cancer signal was detected, but comprehensive medical workups proved there was no cancer present. Because cancer is relatively rare in the general population, even a high 99.1% specificity resulted in the majority of positive tests being wrong; out of the 92 people who had a positive test, 57 (62%) were false positives. For the patient, a false positive means undergoing unnecessary clinic visits, laboratory tests, and advanced imaging. In this study, patients with false positive results waited a median of 162 days before being officially cleared of a cancer diagnosis.
- Sensitivity and False Negatives by Stage: Sensitivity is the test’s ability to correctly flag patients who do have cancer. A false negative occurs when the test reports “no cancer signal detected,” but the patient actually has a tumor. During the 12-month study period, the test resulted in 86 false negatives. While the authors note it is currently infeasible to definitively compare the exact sensitivity of various MCED test methods , the data clearly demonstrates that the test struggles with sensitivity for early-stage disease. Specifically, among the 75 missed new cancers (false negatives), the vast majority (73%, or 55 cases) were early-stage (Stage I or II). Conversely, of the 29 new cancers the test successfully found (true positives), only 48% (14 cases) were Stage I or II. For the non-statistician, this translates to a simple clinical reality: the test is currently much more likely to miss an early-stage cancer than it is to detect it.
Assertive Critical Appraisal
- Limitations & Bias (STROBE Framework): The study population was highly adherent to established cancer screening protocols at baseline. Some participants even received non-standard screening that extends beyond current recommendations. This high background screening rate likely contributed to the high number of false negatives, as many cancers were found by routine mammograms or colonoscopies rather than the experimental blood test. Furthermore, volunteer bias may have influenced the cohort’s overall risk profile or their willingness to undergo extensive diagnostic workups.
- Reporting Quality Assessment (STROBE): The paper provides a clear participant flow diagram and thoroughly describes the subsequent diagnostic pathways taken by the patients. The authors accurately note that the high baseline screening adherence limits the study’s generalizability.
- Applicability: The generalizability of the cancer detection rate is severely constrained by the study cohort’s lack of diversity. The participants were 91.7% non-Hispanic white and were highly educated. Additionally, all costs for advanced imaging and laboratory testing were fully supported by the study sponsor. Because access to advanced diagnostics is often limited by insurance coverage in the real world, the diagnostic timelines seen here may not be reflective of general clinical practice.
- Research Objective: The study aimed to evaluate the feasibility of MCED testing in outpatient settings for adults over age 50 without symptoms of cancer.
- Study Design: This was a prospective cohort study. A convenience sample was consented to testing, and diagnostic evaluations for positive results were coordinated at the discretion of the ordering physician.
- Setting and Participants: The study was conducted in oncology and primary care outpatient clinics across seven U.S. health networks. Eligible participants were adults 50 years or older without current signs or symptoms of cancer. Participants were enrolled both with and without additional cancer risk factors, such as a smoking history or a known cancer predisposition.
Bibliographic Data
- Title: PATHFINDER: A Prospective Cohort Study of Blood-Based Multi-cancer Early Detection
- Authors: Prof. Deborah Schrag, Prof. Tomasz M. Beer, Charles H. McDonnell III, Lincoln Nadauld, Christina A. Dilaveri, Robert Reid, Catherine R. Marinac, Karen C. Chung, Margarita Lopatin, Eric T. Fung, Prof. Eric A. Klein
- Journal: Lancet
- Year: 2023
- DOI: 10.1016/S0140-6736(23)01700-2
Original Article:
Full text: PubMed Central
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.