
Comment:
Medical surveillance fundamentally assumes that earlier detection equates to prolonged survival, making routine imaging an almost sacrosanct practice in oncology. Yet, this nationwide population-based study of non-Hodgkin lymphoma (NHL) survivors exposes an uncomfortable clinical reality: overzealous surveillance computed tomography (CT) drastically increases the risk of secondary primary malignancies (SPMs) without offering a proven overall survival benefit. Although it’s simple to assume they are relatively benign as there is no immediate obvious side effect, this data makes clear that we should treat diagnostic radiation as an active, cumulative exposure requiring rigorous justification.
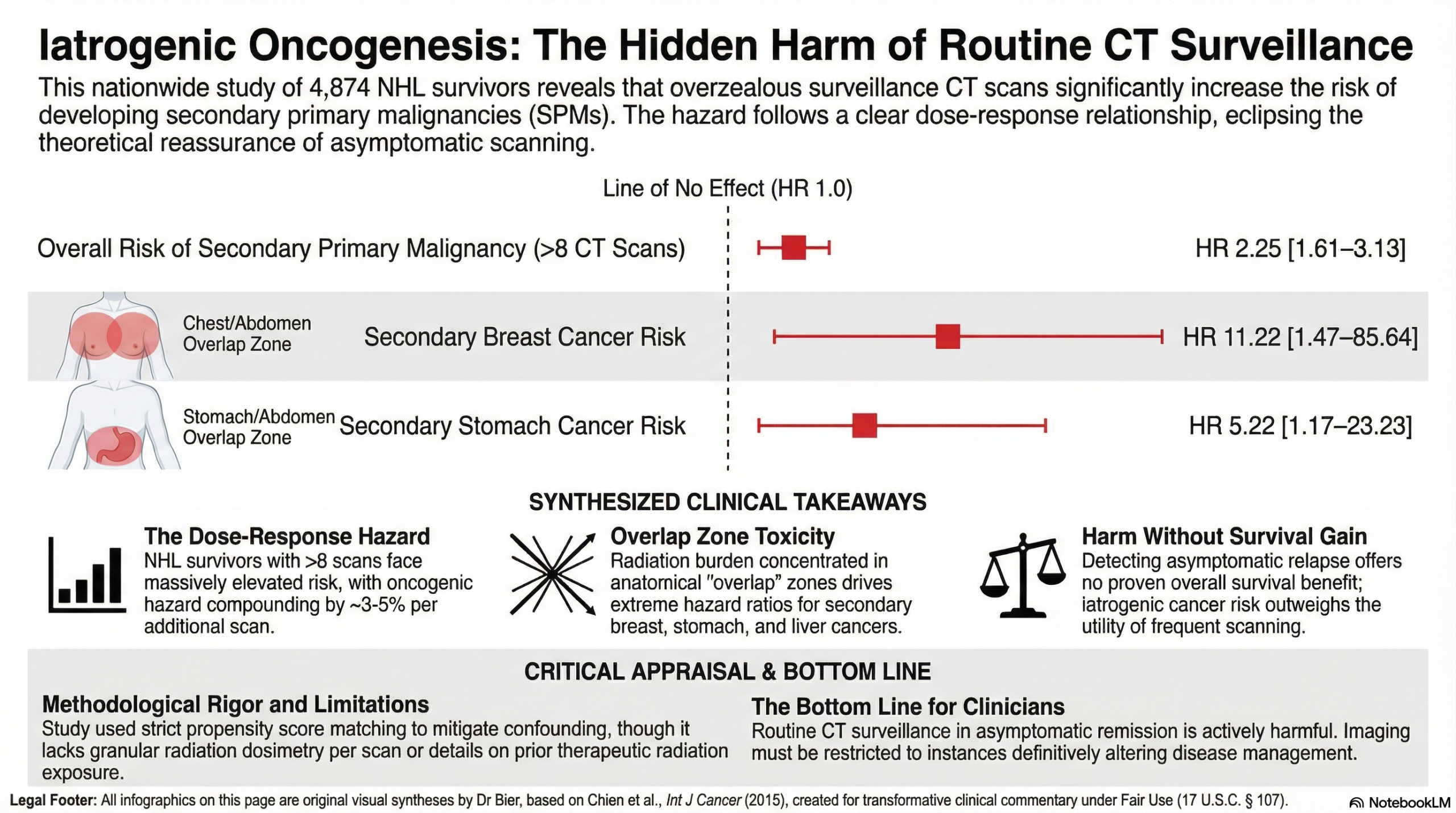
When analyzing 4,874 NHL patients who received curative-intent treatment, the data demonstrates a clear and unforgiving dose-response relationship between imaging frequency and oncogenesis.
-
Patients subjected to more than 8 CT scans in their first year of diagnosis faced a significantly elevated risk of developing a secondary cancer (Hazard Ratio [HR] 2.25, 95% CI 1.61–3.13) compared to those receiving 8 or fewer scans.
-
This risk is not abstract or evenly distributed; it is highly specific to organs often trapped in the radiation “overlap” zones of standard chest and abdominal staging scans.
-
Excessive CT exposure drove a staggering increase in breast cancer (HR 11.22), stomach cancer (HR 5.22), and liver and biliary tract cancers (HR 2.18).
-
The hazard compounds at a rate of roughly 3% to 5% with every single additional scan performed.
-
In patients subjected to 12 or more scans, the risk of a new primary cancer tripled (HR 3.03, 95% CI 2.01–4.57).
Importantly, previous data highlighted within the study confirms that detecting asymptomatic relapse via routine CT surveillance does not translate to an increase in overall survival. Therefore, the theoretical reassurance of an active surveillance schedule is entirely eclipsed by the hard clinical endpoint of iatrogenic harm. For asymptomatic patients who have achieved remission, the default institutional practice of scheduling frequent, routine CT scans is a risk without matching benefit. Accumulating radiation burden is a direct threat to long-term survival, so imaging should be reserved strictly to instances where it will definitively alter disease management.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This large-scale observational study identifies a significant dose-response relationship between the frequency of surveillance CT scans and the development of second primary malignancies (SPMs) in patients with non-Hodgkin lymphoma (NHL). While surveillance imaging is common practice, this study suggests that patients receiving more than 8 CT scans have more than double the risk of developing a new cancer compared to those receiving 8 or fewer scans. Clinicians should weigh the limited survival benefit of routine surveillance CT in asymptomatic patients against this clear, cumulative radiation risk.
Results in Context
- Main Results: NHL patients receiving >8 CT scans had a significantly higher risk of developing an SPM (Hazard Ratio [HR] 2.25; 95% CI 1.61–3.13; p < 0.001) compared to those with ≤8 scans.
- Dose-Response Effect: The risk of SPM was estimated to increase by 3% to 5% for every additional CT scan performed. Patients receiving ≥12 scans showed a three-fold increase in risk (HR 3.03).
- Specific Cancer Risks: Higher CT exposure was specifically associated with significantly increased incidences of:
- Breast Cancer: HR 11.22.
- Stomach Cancer: HR 5.22.
- Liver and Biliary Tract Cancer: HR 2.18.
- Latent Period Analysis: To ensure the CT scans weren’t just detecting existing cancers (surveillance bias), the authors used 1-year and 2-year latent periods; the increased risk remained statistically significant (2-year latent HR 1.036 per scan; p = 0.037).
- Definitions: A Hazard Ratio (HR) of 2.25 indicates that, at any point in time, patients in the high-exposure group were 2.25 times more likely to be diagnosed with a new primary cancer than those in the low-exposure group.
- Participants: Out of 21,600 identified NHL patients, 4,874 met the strict inclusion criteria (received curative-intent CHOP chemotherapy and survived/followed for at least one year).
Assertive Critical Appraisal
- Limitations & Bias (STROBE): The study is retrospective and relies on the Taiwan National Health Insurance Research Database (NHIRD). A major limitation is the lack of data on exact radiation dosages per scan, the specific stages of lymphoma, and prior radiation therapy (RT) exposure, which is a known independent risk factor for SPM.
- Reporting Quality (STROBE): The authors effectively addressed the primary challenge of observational research—confounding—by using Propensity Score Matching. This matched patients in the high and low exposure groups by age, sex, and comorbidities, ensuring the increased cancer risk was specifically associated with the number of CT scans rather than the patients’ baseline health.
- Reporting Quality (RECORD): As a Real-World Evidence (RWE) study, the authors clearly defined “catastrophic illness” certificates as the mechanism for ensuring diagnostic accuracy for both the initial lymphoma and the subsequent SPMs. However, the database lacked specific NHL subtypes (e.g., Diffuse Large B-cell vs. Follicular), which might influence how aggressively a physician orders scans.
- Applicability: The findings are highly relevant to clinical practice. The study highlights that the organs most at risk (breast, stomach, liver) are often located in the “overlap” zones of chest and abdominal CT scans, where radiation doses may effectively double. Given that routine CT surveillance has not been proven to improve overall survival in asymptomatic NHL patients, these results support a more “judicious” approach to imaging.
Research Objective
To investigate whether the frequency of surveillance CT scans in NHL patients who have received curative-intent treatment is associated with an increased risk of developing secondary primary malignancies (SPMs).
Study Design
A nationwide, population-based retrospective cohort study using data from 1997 to 2010. Patients were stratified into two groups based on the median number of CT scans (8) performed within the first year of diagnosis.
Setting and Participants
The study utilized the Taiwan National Health Insurance Research Database (NHIRD), covering 99% of the Taiwanese population. Participants were adults newly diagnosed with NHL receiving standard CHOP-based chemotherapy with at least one year of follow-up.
Bibliographic Data
- Title: Frequency of surveillance computed tomography in non‐Hodgkin lymphoma and the risk of secondary primary malignancies: A nationwide population‐based study
- Authors: Sheng-Hsuan Chien, Chia-Jen Liu, Tzeon-Jye Chiou, Jyh-Pyng Gau, Yu-Wen Hu, Ying-Chung Hong, Chung-Jen Teng, Chiu-Mei Yeh, and Cheng-Hwai Tzeng
- Journal: International Journal of Cancer
- Year: 2015
- DOI: 10.1002/ijc.29433
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.