
Comment:
I have used the free PSA ratio (%fPSA) for years because it provides a reliable, cost-effective method to triage patients hovering in the PSA gray zone without immediately resorting to invasive procedures. Despite it being clear in the literature for decades, it is rare that I see it being used. The relatively recent availability of multiparametric MRIs has added a helpful tool to save men from unnecessary biopsies, however it still, as any tool, has a significant amount of false positive and false negatives. This retrospective analysis confirms that the %fPSA can effectively synergize with the MRI for improved accuracy.
Before the advent of multiparametric MRI, when I utilized the free PSA ratio as a primary standalone screening tool for men in the PSA gray zone, we faced this exact same structural constraint. A serum marker can’t perfectly distinguish between benign glandular hyperplasia and an organ-confined malignancy. When deployed as a generalized first-line screen across all stages, a highly sensitive 25% cutoff successfully flags roughly 95% of cancers, although the cutoff changes with age. Yet, this still guarantees a 5% false-negative rate, meaning we inherently miss one in twenty malignancies. More devastatingly, this threshold carries a massive false-positive rate approaching 80%. Historically, relying exclusively on %fPSA without prior structural imaging meant channeling the vast majority of healthy men into an unnecessary biopsy.
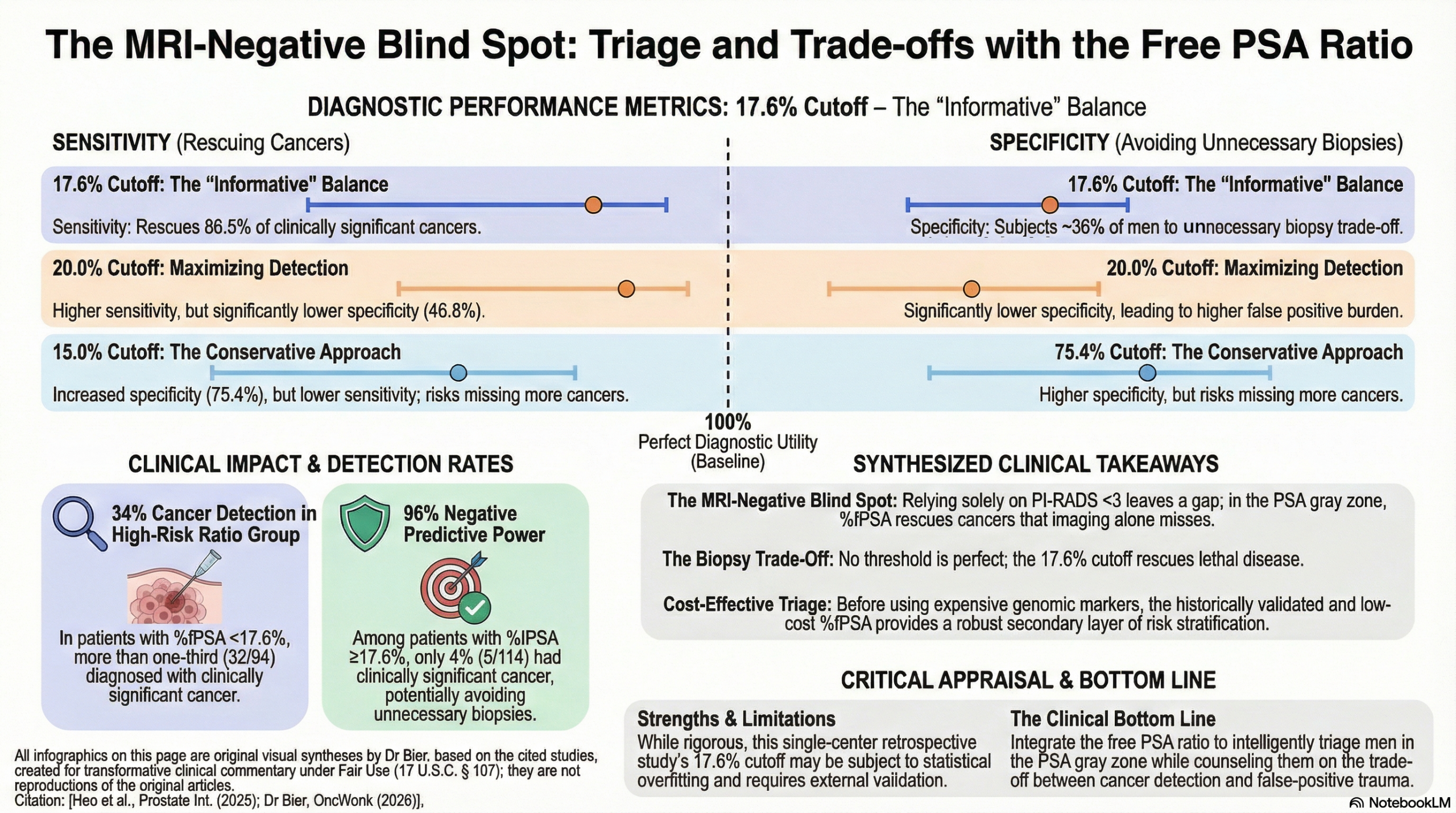
However, analyzing the inherent sensitivity and specificity of %fPSA exposes a profound diagnostic hazard depending on where we set the threshold. If we adopt the traditional 20% cutoff, the assay yields a 91.9% sensitivity but a dismal 46.8% specificity. While this reduces the false-negative hazard (missing only 8.1% of cancers), it balloons the false-positive rate to 53.2%, channeling a massive number of healthy men into an unnecessary biopsy. Tightening the threshold to 17.6% drops the false-positive rate to 36.3%, but forces us to accept a higher 13.5% false-negative rate. The definitive takeaway is that there is no perfect threshold; we must carefully wield %fPSA to balance the necessity of finding lethal disease against the structural trauma of over-biopsying, a pragmatic reality that expensive newer tests have yet to solve.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This diagnostic accuracy study suggests that in men with a “negative” or “low-risk” prostate MRI (PI-RADS <3) and PSA levels in the gray zone (≤10 ng/ml), a free PSA ratio (%fPSA) cutoff of 17.6% can effectively triage patients for biopsy. Implementing this threshold could identify 86.5% of clinically significant cancers (CSC) that might otherwise be missed by relying on MRI alone, while potentially sparing approximately 64% of patients with benign findings from unnecessary invasive procedures. While %fPSA is an older biomarker, this study provides a practical, cost-effective strategy for a common clinical dilemma where expensive newer markers (like PHI or 4K) may not be available.
Results in Context
- Main Results: Using a %fPSA cutoff of 17.6%, the study found a sensitivity of 86.5% and a specificity of 63.7% for detecting CSC.
- Performance Metrics: * Area Under the Curve (AUC): The %fPSA performed significantly better (AUC = 0.757) than total PSA (AUC = 0.393) or absolute free PSA (AUC = 0.611) in this specific patient population.
- Detection Rates: CSC was found in 34% of patients with %fPSA <17.6%, compared to only 4% of patients with %fPSA >17.6%.
- Definitions: * Clinically Significant Cancer (CSC): Defined as Gleason grade group (GGG) ≥ 2.
- PI-RADS <3: Refers to MRI findings where CSC is considered unlikely (scores of 1 or 2).
- Biomarker Context: %fPSA (free PSA divided by total PSA) is a readily available, low-cost serum marker used to differentiate prostate cancer from benign prostatic hyperplasia (BPH).
Assertive Critical Appraisal
- Appraisal of Biomarker Claim: This is a prognostic/diagnostic biomarker study. The authors successfully demonstrate that %fPSA adds value after an MRI has been performed, addressing the clinical gap of “MRI-negative” patients who may still harbor significant disease.
Reporting Quality Assessment (REMARK):
- Strengths: The study clearly specifies the patient population (PI-RADS <3, PSA \le 10), the assay used, and uses ROC analysis to determine the optimal cut-point.
- Weaknesses: As a single-center retrospective analysis, the 17.6% cutoff may be subject to “overfitting” to this specific cohort and requires external validation before being adopted as a universal standard.
- Trade-offs in Cutoffs: The authors compared the 17.6% threshold against traditional 15% and 20% cutoffs.
- 15% cutoff: Higher specificity (75.4%) but lower sensitivity (67.6%), meaning more cancers would be missed.
- 20% cutoff: Higher sensitivity (91.9%) but very low specificity (46.8%), leading to many unnecessary biopsies.
- The 17.6% threshold was selected as the most “informative” based on Likelihood Ratios (LR).
- Applicability: These findings are highly relevant to general urology and primary care. Because %fPSA is significantly cheaper than newer genomic tests or the PHI test, it represents a high-value “triage” step in healthcare systems with limited resources.
Research Objective
To evaluate the diagnostic performance of the free PSA ratio in detecting clinically significant prostate cancer in patients with a PI-RADS score <3 and total PSA levels \le 10 ng/ml.
Study Design
Retrospective diagnostic accuracy study analyzing 1,435 biopsies. A sub-cohort of 208 patients meeting the specific MRI and PSA criteria was used for the primary analysis. All patients underwent systematic biopsy following MRI.
Setting and Participants
- Setting: Single institution (Yonsei University, Seoul, Korea) between April 2018 and January 2023.
- Participants: Men with PI-RADS <3 and PSA between 4 and 10 ng/ml.
- Median Age: 65 years.
- Median PSA: 5.06 ng/ml.
Bibliographic Data
- Title: Usefulness of free PSA ratio to enhance detection of clinically significant prostate cancer in patients with PI-RADS<3 and PSA≤10
- Authors: Ji Eun Heo, Hyun Ho Han, Won Sik Jang, Won Sik Ham, Woong Kyu Han, Young Deuk Choi, Jongsoo Lee
- Journal: Prostate International
- Year: 2025
- DOI: https://doi.org/10.1016/j.prnil.2024.12.001
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.