
Comment:
While this data from the ‘donna’ program shows a statistically significant survival advantage for screened patients, we can’t conflate ‘survival’ with ‘reduced mortality.’ The study design focuses on women already diagnosed with breast cancer, which inherently makes the results susceptible to lead-time bias—where earlier detection creates an illusion of longer survival without necessarily changing the date of death. Furthermore, the ‘healthy user effect’ is a major confounder here; women who participate in screening programs typically have better baseline health and socioeconomic status, which likely contributes to their improved outcomes independent of the screening itself.
And it tells us nothing about the health and overall survival of the total screened population compared to the unscreened. Whether mammography screening improves overall survival is not addressed.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This retrospective cohort study demonstrates that women diagnosed with breast cancer within the “donna” screening program experienced significantly prolonged overall and breast cancer-specific survival compared to women diagnosed outside the program. However, it is critical to distinguish that this study examined survival rates only among women already diagnosed with breast cancer, rather than breast cancer mortality across the entire eligible population.
Because the study compares survival time from the point of diagnosis, the results are inherently susceptible to lead-time bias (where earlier detection makes survival appear longer without necessarily changing the date of death) and length bias (where screening tends to detect slower-growing, less aggressive tumors). While the authors attempted to statistically correct for these biases, the fundamental design limitation remains: a survival benefit in diagnosed patients does not automatically equate to a reduction in population mortality.
Results in Context
Main Results
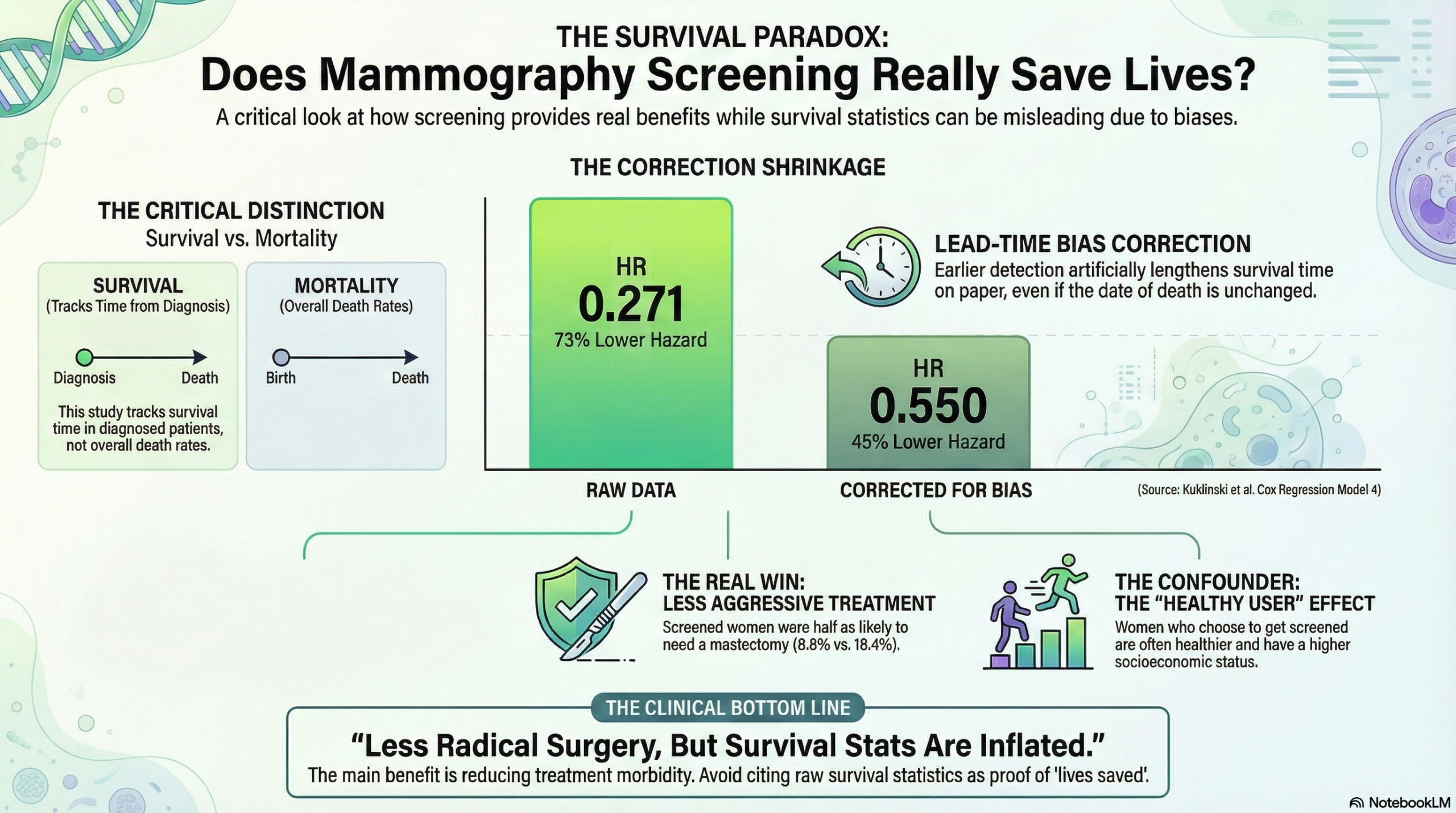
- Unadjusted Survival: Women diagnosed within the Mammography Screening Program (MSP) had a significantly lower hazard of mortality compared to those outside the program, with an unadjusted Hazard Ratio (HR) of 0.271 (95% CI 0.197–0.369).
- Lead-Time Corrected Survival: After correcting for lead-time bias and adjusting for age, tumor size, and Ki-67 proliferation index, the MSP group still maintained a survival advantage, with an HR of 0.550 (95% CI 0.389–0.778) for overall survival.
- Tumor Characteristics: Cancers detected within the MSP were significantly smaller (mean 19.1 mm vs. 24.9 mm) and diagnosed at earlier stages (46.5% Stage I vs. 33.0% outside the MSP) compared to those detected outside the program.
- Treatment Burden: Women in the MSP group underwent fewer radical mastectomies (8.8% vs. 18.4%) and less frequently required adjuvant chemotherapy (33.7% vs. 44.1%).
Definitions
- Hazard Ratio (HR): An HR of 0.550 indicates that, at any given time point, the rate of death in the MSP group was roughly 45% lower than in the non-MSP group, after statistical adjustments.
- Lead-Time Bias: The artificial lengthening of survival time caused by detecting the cancer earlier in its course, even if the time of death remains unchanged.
- Participants: The final analysis included 1,057 breast cancer cases within the MSP and 1,501 cases outside the MSP.
Assertive Critical AppraisalLimitations & Bias (STROBE Framework)
- Selection Bias (Healthy User Effect): The “Outside MSP” group consists of women who either chose not to screen or were screened opportunistically. The authors acknowledge that women who participate in screening often have higher socioeconomic status and different health behaviors than non-participants. These unmeasured confounders likely contribute to the survival difference independent of the screening itself.
- Survival vs. Mortality: The most significant limitation is the metric itself. Evaluating survival of cases rather than mortality of the population invariably favors screening due to the biases mentioned below.
- Residual Lead-Time and Length Bias: Although the authors applied Duffy’s method to correct for lead-time and controlled for Ki-67 (a marker of cell proliferation) to address length bias, these are mathematical estimations. They cannot fully eliminate the fact that screening preferentially identifies indolent, slow-growing cancers that have a better prognosis regardless of treatment.
- Overdiagnosis: The authors excluded in-situ carcinomas (DCIS) to account for overdiagnosis. However, invasive cancers can also be overdiagnosed (detecting cancers that would never have caused symptoms), contributing to the inflated survival numbers in the screened group.
Reporting Quality Assessment (STROBE/RECORD)
- The reporting is generally strong. The authors clearly utilized registry data linkage and were transparent about their statistical methods for handling lead-time bias.
- They adequately described the differences in treatment pathways (e.g., higher use of certified breast centers for MSP patients), which is a crucial meaningful variable that explains some of the survival benefit independent of early detection.
Applicability
The findings are highly relevant to the Swiss healthcare context and confirm that organized screening leads to less aggressive treatment (less mastectomy/chemotherapy). However, clinicians should be cautious about interpreting the magnitude of the survival benefit (HR 0.271 unadjusted) as a direct reflection of lives saved, as it is heavily influenced by the “healthy screener” and lead-time effects.
Research Objective
The study aimed to compare the tumor stage distribution, treatment characteristics, and survival rates of women with breast cancer detected within the “donna” mammography screening program versus those detected outside the program.
Study Design
- Design: Retrospective cohort study.
- Methodology: Data merger between the MSP “donna” database and the Cancer Registry of Eastern Switzerland.
- Adjustments: Analyses were corrected for lead-time bias using mean sojourn times and adjusted for incidence period to account for treatment advancements.
Setting and Participants
- Setting: The Swiss cantons of St. Gallen and Grisons.
- Period: Diagnoses occurring between 2010 and 2019.
- Population: Women aged 50 to 69 diagnosed with invasive (ICD-10: C50) or in-situ (D05) breast cancer.
Bibliographic Data
- Authors: Kuklinski D, Blum M, Subelack J, Geissler A, Eichenberger A, Morant R.
- Title: Breast cancer patients enrolled in the Swiss mammography screening program “donna” demonstrate prolonged survival
- Journal: Breast Cancer Research
- Year: 2024
- DOI: 10.1186/s13058-024-01841-6
Original Article:
Full text: PubMed Central
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.