
Comment:
This is a weak study in numerous ways, with large heterogenicity and a significant results borne of several non-significant studies which always makes it suspect.
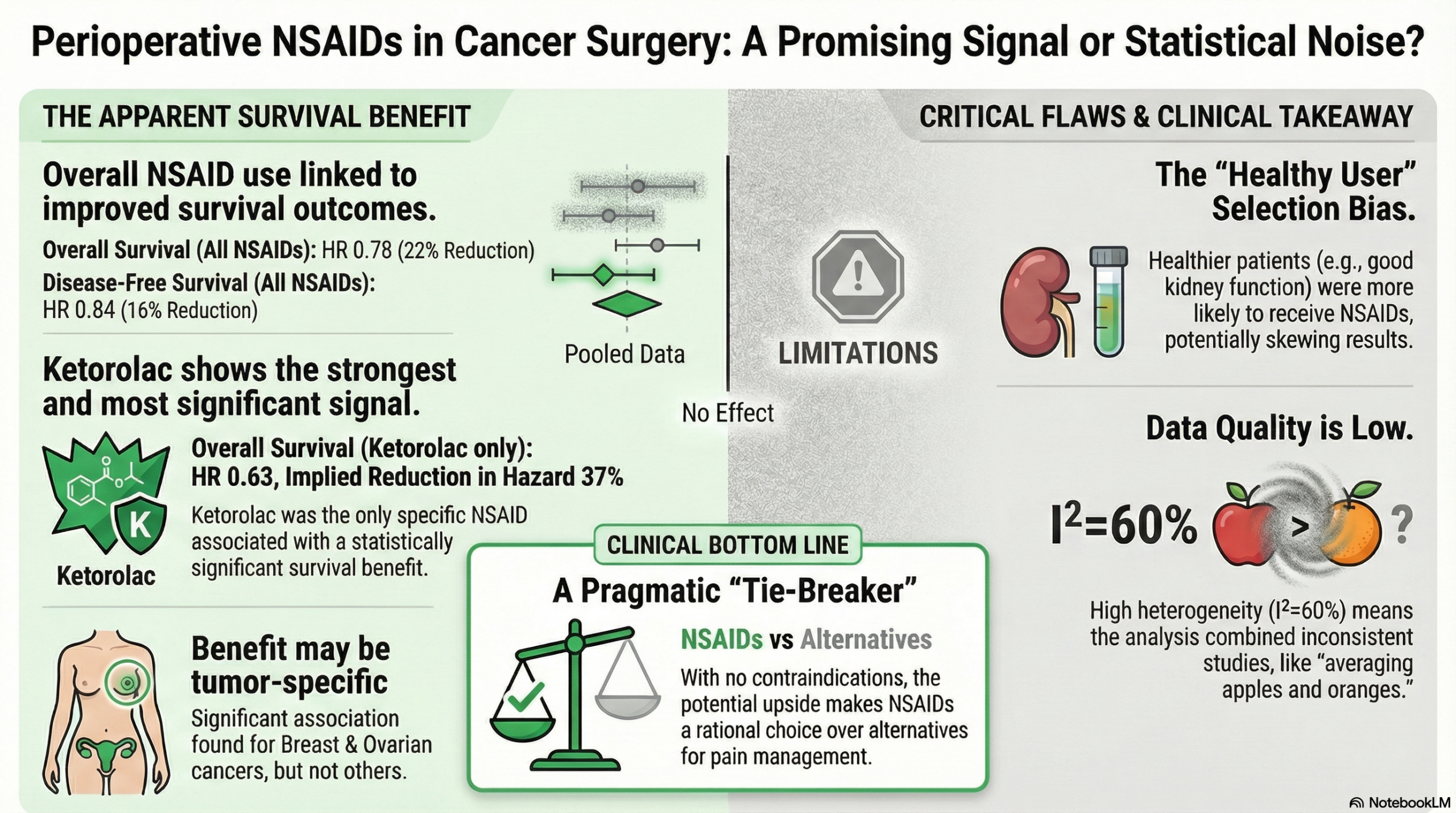
And if a patient has no contraindications, choosing an NSAID over acetaminophen if pain control is needed seems like the clear winner.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This systematic review and meta-analysis suggests that the use of perioperative NSAIDs is associated with improved Disease-Free Survival (DFS) and Overall Survival (OS) in patients undergoing cancer surgery. Specifically, the drug ketorolac showed a significant association with improved overall survival. However, the certainty of this evidence is rated as Low. The positive findings are largely driven by retrospective observational studies with significant heterogeneity, meaning the results could be influenced by selection bias (e.g., healthier patients receiving NSAIDs) rather than the drug itself. Therefore, while the signal is promising, these findings should be considered hypothesis-generating rather than practice-changing until confirmed by large prospective trials.
Results
- Summary of Results:
- Disease-Free Survival (DFS): The pooled analysis showed a statistically significant benefit for NSAID users, with a Hazard Ratio (HR) of 0.84 (95% CI, 0.73–0.97). This indicates a 16% reduction in the hazard of disease recurrence or death compared to controls.
- Overall Survival (OS): There was a significant benefit for NSAID users, with an HR of 0.78 (95% CI, 0.64–0.94), representing a 22% reduction in the hazard of death.
- Ketorolac Specifics: In subgroup analyses, ketorolac was the only specific NSAID associated with a significant improvement in Overall Survival (HR 0.63; 95% CI, 0.42–0.95).
- Cancer Type: Significant associations with longer DFS were observed in breast and ovarian cancer subgroups, but not in lung, colorectal, or prostate cancers.
Assertive Critical Appraisal
- Certainty of Evidence (GRADE Framework): The authors explicitly rated the certainty of evidence as Low for both DFS and OS. This downgrade is appropriate and primarily due to the “risk of bias in studies, high heterogeneity, and imprecise definitions” inherent to the retrospective data included.
- Heterogeneity:
- The analysis reported an I² of 60% for the primary outcome of Disease-Free Survival. This indicates substantial heterogeneity, meaning the variation in results across studies is likely due to real differences in study populations, NSAID protocols, or cancer types rather than just chance. Consequently, the pooled average should be interpreted with caution.
- Heterogeneity was particularly high in the breast cancer subgroup (I²=77%).
- Risk of Bias in Included Studies: The majority of included studies (15 out of 19) were retrospective cohorts. This introduces a high risk of selection bias; for example, surgeons may have avoided NSAIDs in patients with significant comorbidities (renal issues, bleeding risk), making the control group sicker at baseline. While most studies attempted multivariate adjustments, residual confounding remains a major threat to validity.
- Special Consideration for Pooled Results: It is important to note that while the overall pooled result is statistically significant, this conclusion is derived from a collection of smaller studies, many of which did not find a significant effect on their own. For instance, in the DFS forest plot, 7 cohorts favored non-NSAID use (crossing the line of no effect), and only 7 of 13 favorable cohorts were statistically significant individually. By combining these data, the meta-analysis increases power, but if the individual retrospective studies share common biases, the meta-analysis simply reinforces that bias.
- Reporting Quality Assessment (PRISMA): The review demonstrates good reporting quality. It adhered to PRISMA guidelines, including a clear flow diagram (Fig. 1) and a registered protocol on Prospero. The search strategy was transparent and provided in the appendix.
- Publication Bias: The authors acknowledge the risk of publication bias, noting that unpublished data unfavorable to the intervention may not have been reported. They do not explicitly report a statistical test (e.g., Egger’s test) to quantify this risk in the provided text.
Research Objective
To investigate the association between perioperative NSAID use and long-term outcomes (DFS and OS) in cancer surgery patients, and to determine if this association is dependent on cancer type, specific NSAID, or timing of administration.
Study Design
- Design: Systematic review and meta-analysis of human studies (RCTs and observational).
- Search: Searched Ovid Medline, Cochrane database, and ClinicalTrials.gov up to January 2021.
- Selection: Two independent reviewers screened titles/abstracts and full texts.
Setting and Participants
- Included Studies: 19 studies were included in the qualitative synthesis, with 16 providing sufficient data for meta-analysis.
- Population: A total of 12,994 participants undergoing surgery with curative intent for various cancers (breast, lung, kidney, prostate, colorectal, ovarian, etc.).
Bibliographic Data
- Title: Perioperative NSAIDs and Long-Term Outcomes After cancer Surgery: a Systematic Review and Meta-analysis
- Authors: Shaji S, Smith C, Forget P.
- Journal: Current Oncology Reports
- Year: 2021
- DOI:10.1007/s11912-021-01133-8
This AI-generated analysis is for informational and research purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of a qualified health provider with any questions you may have regarding a medical condition.
Original Article:
Full text: PubMed Central
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.