
Comment:
The traditional clinical focus on “detecting cancer early” ignores the historical trajectory of screening evidence, where every rigorous randomized trial has failed to demonstrate a statistically significant improvement in all-cause mortality. While this study reports that longer screening intervals are associated with “substantially worse OS,” we should recognize that this observational signal is notoriously unstable and subject to unmeasured confounding that statistical models cannot eliminate. These findings are a likely fueled by Healthy User Bias. Women who adhere to strict annual imaging typically possess superior baseline metabolic profiles and higher socioeconomic status—variables that drive survival entirely independent of the mammogram itself. What wasn’t accounted for?
-
Metabolic Integrity: The study did not adjust for Body Mass Index (BMI) or metabolic health markers (e.g., HbA1c or blood pressure). Annual screeners are more likely to manage these variables, reducing their risk of death from CVD—the leading competitor for mortality in these age groups.
-
Preventative Proactivity (The “Scout” Effect): Adherence to annual mammography is a surrogate for adherence to all preventative care. These women likely have higher rates of statins usage, colorectal screening, and exercise adherence. The mammogram is not saving them; their lifestyle is.
-
Educational and Socioeconomic Resilience: The authors adjusted for “race” but not for Educational Attainment or Household Income. These are non-negotiable drivers of All-Cause Mortality that influence survival through better nutrition, lower chronic stress, and superior post-diagnosis support.
-
Toxic Habits: By failing to control for Smoking Status or Alcohol Consumption, the study ignores the two most potent variables for secondary cancers (lung, esophageal) and cardiovascular catastrophe.
The study has likely mistaken a marker of health for a cause of health. In an average-risk population, annual screening adherence is less a medical intervention and more a demographic identifier of low-risk individuals. To claim an Overall Survival benefit without accounting for BMI, smoking, or socioeconomic resilience is to ignore the primary drivers of human longevity.
For years, I have cautioned that disease-specific survival is a biased metric, and claiming an all-cause mortality benefit based on retrospective data—without controlling for confounding variables such as comorbidities or smoking status—is a leap we should be skeptical of. The tradeoff between harm and benefit for regular mammography screening has been shifting toward harm for decades, and this study doesn’t substantially change that.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This retrospective observational cohort study reports that annual mammography screening is strongly associated with improved overall survival compared to less frequent screening intervals. However, because this is an observational study evaluating overall (all-cause) survival rather than breast cancer-specific survival, the reported survival benefits are highly likely to be overstated. The discrepancy between these findings and rigorous randomized controlled trials (RCTs) is largely driven by unmeasured confounding factors—such as healthy user bias—and inherent screening biases that statistical models cannot fully eliminate.
Results in Context
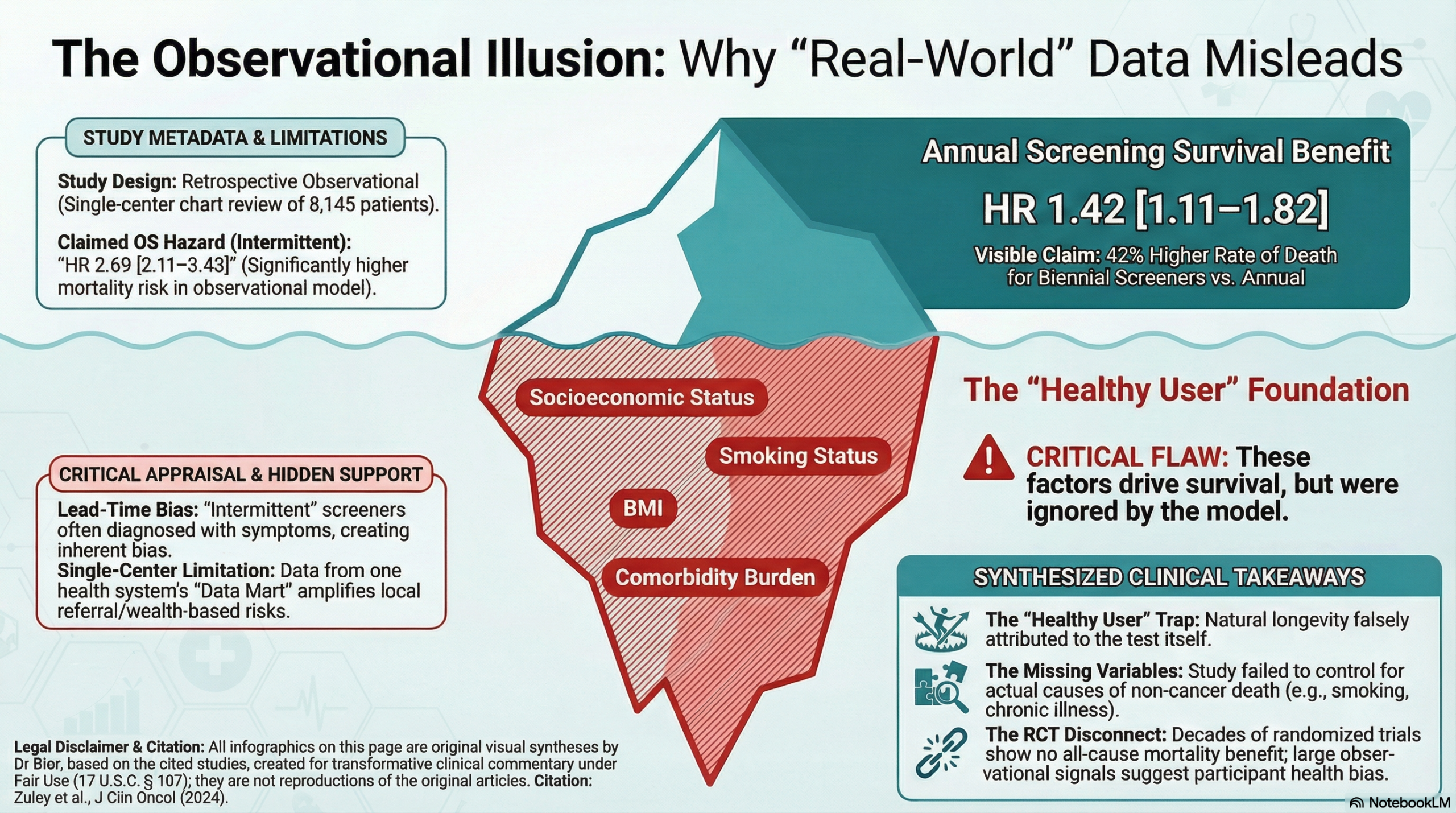
- Main Results: The study found that, compared to annual screening, biennial (every two years) screening was associated with a relative hazard of 1.42 (95% CI: 1.11-1.82) for overall survival, meaning worse survival. Intermittent screening (>27 months) was associated with a relative hazard of 2.69 (95% CI: 2.11-3.43), indicating significantly worse overall survival. After the authors adjusted for potential lead-time bias by analyzing survival from a uniform fixed timepoint, the hazard ratios remained elevated at 1.39 (95% CI: 1.08-1.78) for biennial and 2.01 (95% CI: 1.58-2.55) for intermittent screening.
- Definitions: A hazard ratio (HR) of 1.42 means that patients in the biennial screening group had a 42% higher rate of death from any cause over the study period compared to patients in the annual screening group.
- Participants: The final analysis included 8,145 patients aged 40 and older who had at least one screening examination prior to their breast cancer diagnosis. The cohort was divided into “annual” (3,369 patients), “biennial” (1,340 patients), “intermittent” (1,129 patients), and “baseline” (2,307 patients) screening adherence groups.
Assertive Critical Appraisal
- Limitations & Bias (STROBE Framework): The primary structural flaw in using an observational dataset to claim an overall survival benefit from a single cancer screening intervention is the massive risk of healthy user bias . Women who strictly adhere to annual mammography screening typically have better overall health behaviors, fewer severe comorbidities, higher socioeconomic status, and better access to systemic healthcare. These unmeasured variables dramatically reduce all-cause mortality entirely independent of breast cancer. The authors themselves explicitly concede that evaluating baseline health across the population was outside the scope of their project and could theoretically confer a bias toward those participating in more frequent screening. Because RCTs randomize these exact confounders equally between groups, they rarely show overall survival benefits for breast cancer screening, focusing instead on disease-specific survival.
- Furthermore, observational screening studies are highly susceptible to length-time bias and lead-time bias . Lead-time bias occurs when a test detects a cancer earlier, artificially increasing the survival time measured from the date of diagnosis, even if the patient’s actual date of death does not change. While the authors attempted to address unobserved differential lead time by comparing post-diagnosis survival from a fixed date for all women rather than individual diagnosis dates, statistical adjustments in retrospective cohorts are imperfect and cannot substitute for the randomized structure of a clinical trial.
- Reporting Quality Assessment (STROBE): The paper fails to clearly describe efforts to address crucial sources of clinical confounding. The authors used multivariable logistic regression and proportional hazards models to adjust for age, race, menopausal status, and first-degree relatives with breast cancer. However, they did not control for major determinants of overall survival such as patient comorbidities, body mass index, smoking status, or socioeconomic markers, which is a major flaw when assessing all-cause mortality.
- Reporting Quality Assessment (RECORD): The study used routinely collected data from an institutional research breast data mart encompassing electronic medical records, radiology information systems, pathology databases, and a cancer registry. The authors adequately described the participant selection process using a cohort development flowchart.
- Applicability: The data reflect real-world screening behaviors within a single organization featuring academic and community medical centers in rural, suburban, and urban settings. However, due to the severe methodological limitations inherent in assessing overall survival via an observational screening cohort, these specific survival findings cannot reliably inform broad clinical practice or override established RCT data.
- Research Objective: The purpose of the study was to evaluate the late-stage cancer rate and overall survival for different screening intervals using a real-world institutional research data mart.
- Study Design: This was a retrospective observational review.
- Setting and Participants: The study utilized data from a single institution’s cancer registry for patients diagnosed with breast cancer between January 1, 2004, and December 31, 2020. The final cohort consisted of 8,145 patients aged 40 and older who had a pre-diagnosis screening history.
Bibliographic Data
- Title: Breast Cancer Screening Interval: Effect on Rate of Late-Stage Disease at Diagnosis and Overall Survival
- Authors: Margarita L. Zuley, Andriy I. Bandos, Stephen W. Duffy, Durwin Logue, Rohit Bhargava, Priscilla F. McAuliffe, Adam M. Brufsky, Robert M. Nishikawa
- Journal: Journal of Clinical Oncology (J Clin Oncol)
- Year: 2024
- DOI: 10.1200/JCO.24.00285
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.