
Comment:
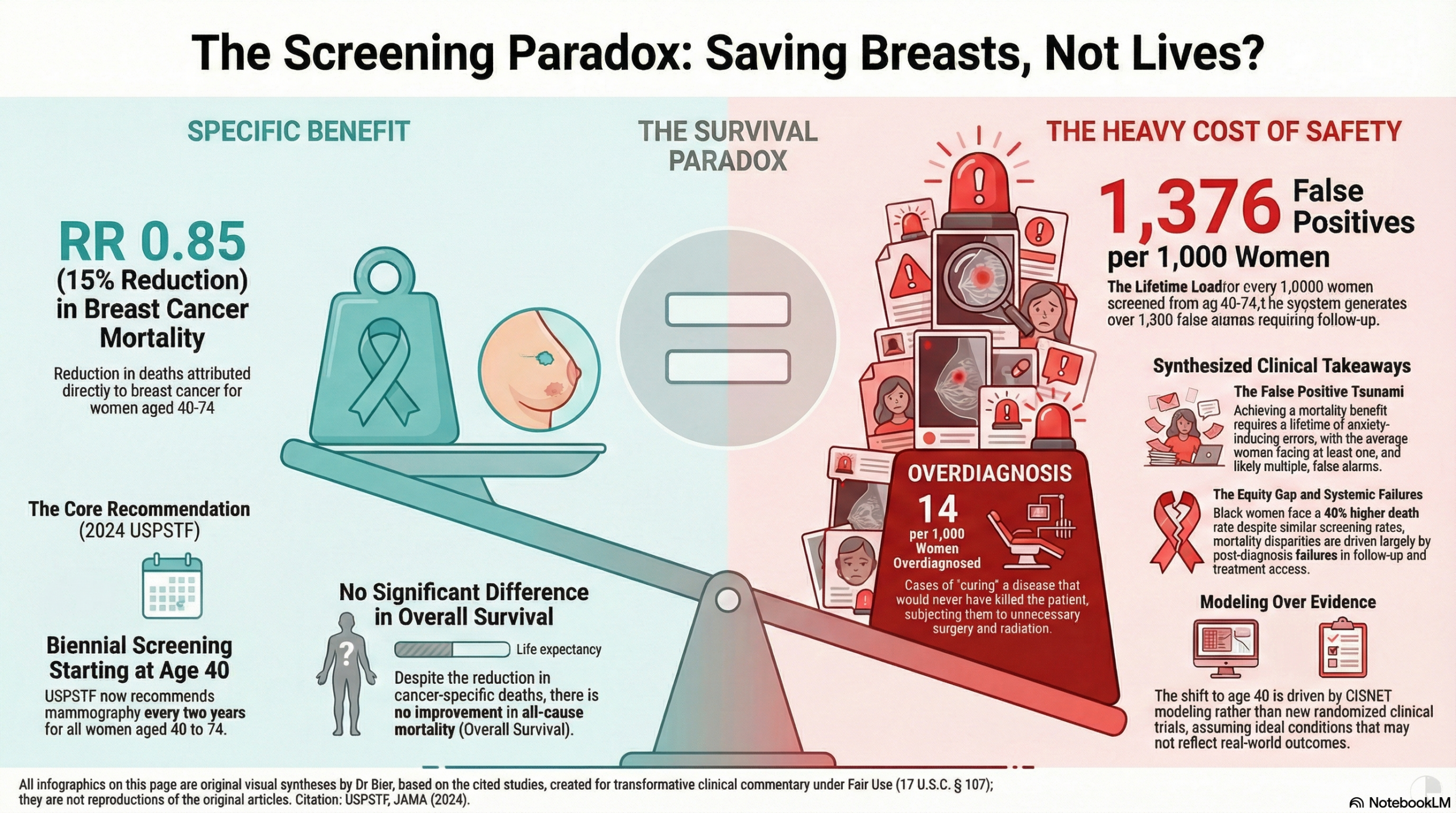
The traditional clinical focus and mantra of “early detection saves lives” ignores the underlying reality that “saving a life from breast cancer” does not equate to “lengthening that patient’s life.” This updated USPSTF recommendation highlights a persistent survival paradox: despite decades of technological advancement, screening mammography has never demonstrated a difference in all-cause mortality. We should be deeply skeptical of an intervention that requires a lifetime of screening to generate 1,376 false positives and 14 overdiagnosed cases per 1,000 women without moving the needle on overall survival.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
The USPSTF recommends biennial screening mammography for all women aged 40 to 74 years to reduce breast cancer mortality. While this strategy significantly improves breast-cancer-specific survival, it is critical to note that current evidence does not demonstrate an improvement in overall survival (OS). This means that while screening reduces the likelihood of dying specifically from breast cancer, it has not been shown to extend the total lifespan of the screened population when accounting for all causes of death. For clinicians, this underscores a “trade-off” : the benefit of averted breast cancer deaths must be weighed against harms like overdiagnosis (14 cases per 1000) and false positives (1376 per 1000), which can lead to invasive procedures for lesions that might never have caused clinical harm.
Results in Context
Primary Outcome: Breast Cancer Mortality vs. Overall Survival
- Breast Cancer Mortality (Specific Survival): Meta-analysis shows a relative risk (RR) reduction in breast cancer death of 0.85 (15%) for women aged 40 to 74 years.
- Overall Survival (OS): No randomized clinical trials (RCTs) or meta-analyses have demonstrated a statistically significant difference in all-cause mortality (Overall Survival) with screening mammography.
- Clinical Significance of the Distinction: An improvement in breast-cancer-specific survival without an increase in OS suggests that the number of lives saved from breast cancer may be offset by other causes of death in the population, or that the absolute number of deaths prevented is too small to shift the needle on total mortality within the study periods.
Key Findings by Subgroup and Modality
- Age 40-49: New evidence, including a 2.0% annual increase in incidence since 2015, led to the “B” recommendation for starting at age 40. Modeling estimates 1.3 additional breast cancer deaths averted per 1000 women by starting at 40 rather than 50.
- Black Women: This population faces a 40% higher mortality rate despite similar screening rates. Modeling suggests starting at age 40 averts 1.8 additional deaths per 1000 Black women, a higher absolute benefit than the general population.
- Digital Breast Tomosynthesis (DBT): 3D mammography shows similar mortality benefits to 2D but may result in fewer false positives (167 fewer per 1000).
Harms and Adverse Events
- False Positives: The most common harm; biennial screening from 40-74 results in 1376 false positives per 1000 women over a lifetime.
- Overdiagnosis: Approximately 11% to 19% of screen-detected cancers may be overdiagnosed—finding lesions (like some DCIS) that would never have caused symptoms or death.
Assertive Critical Appraisal
Certainty of Evidence (GRADE-style Assessment)
- Moderate Certainty: The USPSTF is moderately certain of a moderate net benefit for biennial screening in ages 40-74.
- Insufficient Evidence (I Statements): Evidence is currently inadequate to determine the balance of benefits/harms for:
- Women 75 years or older (no RCTs included this age group).
- Supplemental screening (MRI/Ultrasound) for women with dense breasts.
The “Survival” Paradox
- Observation: The primary metric of success in these guidelines is “breast cancer deaths averted”. However, the failure to move the OS marker is a significant caveat for patient counseling.
- Statistical Rationale: Breast cancer deaths, while a leading cause of cancer death, represent a fraction of total annual deaths. Detecting a shift in OS requires massive sample sizes and decades of follow-up, which most trials lack.
- Critical Caveat: Clinicians must be aware that “saving a life from breast cancer” does not always equate to “lengthening that patient’s life” if they are at risk for competing causes of death, particularly in older cohorts or those with significant comorbidities.
Reporting Quality and Applicability
- Modeling vs. Empirical Data: Much of the new recommendation (especially for age 40 and Black women) relies on collaborative modeling rather than new RCTs. While modeling helps fill gaps, it relies on assumptions about treatment efficacy and screening adherence that may not reflect real-world local practice.
- Equity Gap: The USPSTF acknowledges that “screening alone will not remedy inequity”. The 40% higher mortality in Black women is tied to post-screening factors: delays in follow-up and inequities in treatment quality.
Research Objective
To update the 2016 recommendation by evaluating the effectiveness of different mammography-based screening strategies (age, interval, modality) on breast cancer incidence, morbidity, and mortality.
Study Design
Systematic Review and Collaborative Modeling. The USPSTF commissioned a systematic review of RCTs and observational studies, supplemented by 6 independent modeling teams (CISNET) to estimate lifetime benefits and harms.
Setting and Participants
Cisgender women and persons assigned female at birth aged 40 or older at average risk (including those with family history or dense breasts, but excluding high-risk genetic syndromes like BRCA1/2).
Bibliographic Data
- Title: Screening for Breast Cancer: US Preventive Services Task Force Recommendation Statement
- Authors: US Preventive Services Task Force (Chair: Wanda K. Nicholson, MD, MPH, MBA)
- Journal: JAMA
- Year: 2024
- DOI: 10.1001/jama.2024.5534
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.