
Comment:
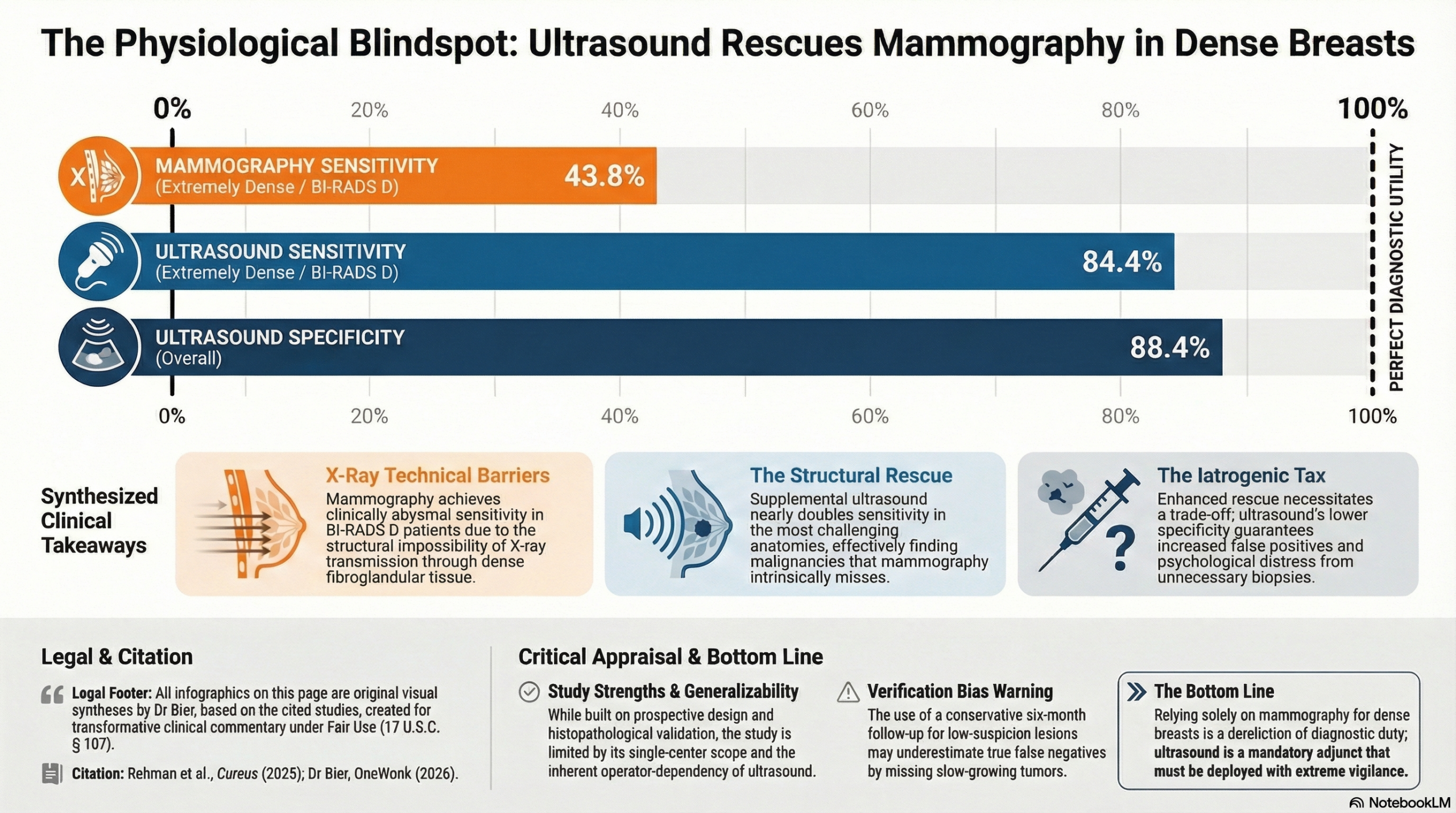
All diagnostic imaging, and really all lab testing, is a series of calculated structural trade-offs – sensitivity vs specificity. In the case of mammograms, it is physiological absurd to rely solely on X-ray transmission to find tumors buried within dense fibroglandular tissue inthat it fundamentally fails to “see” through BI-RADS D breasts. In extremely dense tissue, mammography achieved an extremely poor sensitivity of just 43.8%.
A tumor hidden behind dense functional tissue is a physiological blindspot, not a failure of the technician. Ultrasound rescues this diagnostic failure, pushing overall sensitivity to 85.3%. However, this structural rescue comes at a cost. While ultrasound found the missed lesions, its slightly lower specificity means it generated more false positives, subjecting an increased number of healthy women to an unneeded biopsy. Hopefully someday we will have perfected imaging modalities or algorithms that can perfectly marry structural penetration with absolute specificity, but the definitive takeaway is that we must aggressively deploy ultrasound as an adjunct for dense breasts to prevent missed cancers, provided we remain hyper-vigilant against medicalizing benign architectural noise.
The Wonk Debate – Audio Critique & Clinical Commentary:
Comment:
Clinical Bottom Line
This prospective observational study provides clear evidence that ultrasound is significantly more sensitive than digital mammography for detecting breast cancer in women with radiographically dense breasts. While mammography maintains high specificity (91.9%), its sensitivity drops precipitously in extremely dense tissue (BI-RADS D) to just 43.8%. Clinicians should view ultrasound as an essential adjunct—not just an alternative—in this patient population, as it maintained a high sensitivity ( >84%) regardless of the level of tissue density.
Results in Context
Main Results
The study compared the performance of digital mammography and high-resolution ultrasound against a histopathological “gold standard” in 240 women with dense breasts.
|
Metric |
Mammography |
Ultrasound |
|
Sensitivity |
61.8% |
85.3% |
|
Specificity |
91.9% |
88.4% |
|
PPV |
75.0% |
74.4% |
|
NPV |
85.8% |
93.8% |
|
Overall Accuracy |
83.3% |
87.1% |
Definitions
- Sensitivity: The ability of the test to correctly identify those with the disease (true positive rate).
- Specificity: The ability of the test to correctly identify those without the disease (true negative rate).
- PPV (Positive Predictive Value): The probability that a patient has the disease given a positive test result.
- NPV (Negative Predictive Value): The probability that a patient does not have the disease given a negative test result.
Participants
- Total Enrolled: 240 patients.
- Density Distribution: 142 (59.2%) were BI-RADS C (heterogeneously dense) and 98 (40.8%) were BI-RADS D (extremely dense).
- Malignancy Rate: 68 (28.3%) cases were histologically confirmed as cancer.
Assertive Critical Appraisal
Limitations & Bias (STROBE Framework)
- Verification Bias: A significant methodological concern is that only BI-RADS 4 or 5 lesions underwent biopsy, while BI-RADS 2 or 3 lesions were followed conservatively for only six months. This could lead to an underestimation of false negatives if slow-growing cancers were missed during the short follow-up period.
- Operator Dependency: The study acknowledges that ultrasound is highly operator-dependent. While the researchers used experienced radiologists and a consensus-reading model to mitigate this, these results may not be reproducible in settings with less specialized staff.
- Single-Center Design: Conducted at a single hospital in Pakistan, the findings might be influenced by local population characteristics or specific equipment, potentially limiting generalizability to other healthcare systems.
Reporting Quality Assessment (STROBE)
The authors generally followed STROBE principles, though there was limited detail on how they addressed potential confounding factors beyond breast density. They did, however, clearly describe the “masking effect” where dense glandular tissue obscures masses on mammograms, providing a biological rationale for the observed sensitivity gap.
Applicability
The findings are highly relevant for clinicians managing women with dense breasts. The high NPV of ultrasound (93.8%) is particularly useful for “ruling out” malignancy and reducing patient anxiety in a primary care setting. Furthermore, the study highlights ultrasound as a cost-effective alternative to MRI or tomosynthesis in resource-limited regions.
Research Objective
To evaluate and compare the sensitivity, specificity, and overall accuracy of ultrasound and mammography in detecting breast cancer specifically within BI-RADS C and D breast density categories.
Study Design
A prospective, comparative observational study conducted between June 2023 and January 2024. All participants received both imaging modalities within a seven-day interval to ensure diagnostic consistency.
Setting and Participants
- Location: Family Health Hospital, Islamabad, Pakistan.
- Criteria: Females aged 30–70 with radiographically dense breasts.
- Exclusions: Women with fatty breast tissue (BI-RADS A/B), prior history of breast cancer/surgery, or those who were pregnant or lactating.
Bibliographic Data
- Title: Comparison of Diagnostic Accuracy of Ultrasound and Mammography in Detecting Breast Cancer in Radiographically Dense Breasts
- Authors: Haseena Rehman, Irshad Ahmad, Saman Rashid, Muqadas Mukhtar, Aftab Ahmad Khan, Huma Khaliq
- Journal: Cureus
- Year: 2025
- DOI: 10.7759/cureus.92637
Original Articles:
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.