
Comment:
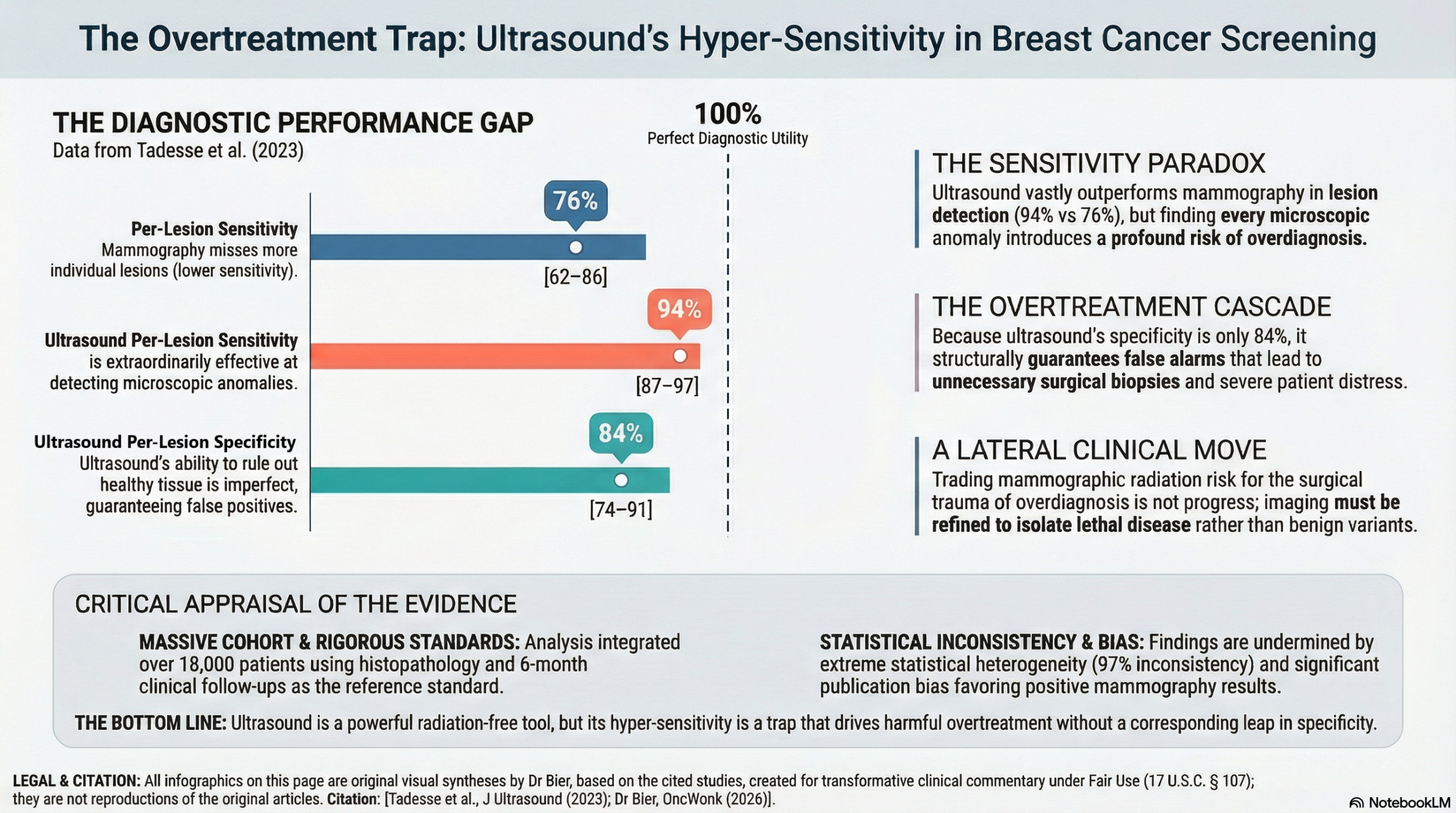
Whenever possible, I actively steer patients toward ultrasound to bypass the cumulative risks of routine mammographic radiation. Yet, the central tension in evaluating this diagnostic meta-analysis is the stark conflict between the modality’s physical safety profile and the systemic diagnostic hazard it creates. The authors demonstrate that ultrasound delivers a staggering 94% per-lesion sensitivity, far outpacing the 76% achieved by mammography. However extreme diagnostic sensitivity without perfect specificity is a recipe for overtreatment. Finding virtually every microscopic lesion guarantees that we will detect an abundance of non-lethal abnormalities, channeling healthy women into unnecessary biopsies and psychological distress simply because a machine was sensitive enough to see a harmless architectural anomaly. I will always favor ultrasound over mammography to eliminate radiation risk, but the definitive takeaway is that trading radiation-induced harm for the surgical trauma of overdiagnosis is a lateral move. We must refine our imaging thresholds to focus exclusively on clinically significant disease before we can celebrate finding more lesions.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This meta-analysis suggests that ultrasound (US) and mammography (MMG) demonstrate comparable diagnostic performance on a per-patient basis for detecting breast cancer. However, on a per-lesion basis, ultrasound appears superior, showing significantly higher sensitivity (94% vs. 76%) and better overall diagnostic accuracy (AUC 0.91 vs. 0.85). While these results advocate for the utility of ultrasound—particularly in symptomatic patients or those with dense breast tissue—the certainty of the evidence is limited by substantial heterogeneity (I2 up to 97%) and evidence of publication bias within the mammography studies.
Results
Summary of Results
The following table summarizes the pooled diagnostic estimates from the bivariate meta-analysis:
|
Metric |
Mammography (MMG) |
Ultrasound (US) |
|
Per-Patient Sensitivity |
0.82 (95% CI: 0.76–0.87) |
0.83 (95% CI: 0.71–0.91) |
|
Per-Patient Specificity |
0.84 (95% CI: 0.73–0.92) |
0.84 (95% CI: 0.74–0.91) |
|
Per-Lesion Sensitivity |
0.76 (95% CI: 0.62–0.86) |
0.94 (95% CI: 0.87–0.97) |
|
Per-Lesion Specificity |
0.82 (95% CI: 0.66–0.91) |
0.84 (95% CI: 0.74–0.91) |
|
Area Under Curve (AUC) |
0.8933 (Per-patient) |
0.8310 (Per-patient) |
|
AUC (Per-Lesion) |
0.8503 |
0.9138 |
- Sensitivity: The ability of the test to correctly identify patients with breast cancer.
- Specificity: The ability of the test to correctly identify patients without breast cancer.
- AUC: A global measure of diagnostic accuracy, where 1.0 is a perfect test.
Assertive Critical Appraisal
Certainty of Evidence (GRADE)
The overall certainty of evidence is Low. While the authors used the QUADAS tool to assess quality, several factors necessitate a downgrade:
- Risk of Bias: MMG studies were of “moderate” quality, with several failing to report withdrawals or uninterpretable results.
- Inconsistency: Extremely high heterogeneity across all primary outcomes.
- Publication Bias: Significant bias was detected for MMG studies.
Heterogeneity
The reported I2 values ranged from 80.2% to 97.2% across the different analyses. I2 represents the percentage of variation across studies due to real differences (such as different patient populations or equipment) rather than chance. An I2 of 97% indicates massive heterogeneity, suggesting the primary studies showed widely different results and the pooled average must be interpreted with extreme caution.
Publication Bias
The authors assessed publication bias using Deeks’ funnel plots and Egger’s test. They found significant publication bias for mammography (per-patient basis), although not for ultrasound. Publication bias is a common threat where studies with “negative” or less impressive results are less likely to be published, potentially leading to an overestimation of a test’s diagnostic performance.
Special Consideration for Pooled Results
It is important to note that while the overall pooled results suggest high sensitivity for ultrasound (94% per-lesion), this conclusion is derived from a collection of studies where individual results varied significantly. This scenario often occurs when individual studies use different thresholds for what constitutes a “positive” finding, a “threshold effect” that was prominent in the ultrasound data (correlation of -0.8085).
Reporting Quality Assessment (PRISMA)
The study demonstrates high reporting quality according to PRISMA principles. The authors included a clear PRISMA flow diagram and detailed their full search strategy, including specific Boolean operators for the PubMed database.
Research Objective
To compare the diagnostic performance (sensitivity, specificity, and accuracy) of mammography and ultrasound in detecting breast cancer.
Study Design
- Type: Systematic review and meta-analysis of diagnostic accuracy studies published between 2008 and 2021.
- Search Strategy: PubMed, Scopus, and EMBASE databases.
- Reference Standard: Histopathologic analysis or clinical/imaging follow-up for at least 6 months.
Setting and Participants
- Total Studies: 24 articles (19 for MMG, 20 for US).
- Total Participants: 18,203 patients.
- Criteria: Women over age 18 undergoing diagnostic imaging for breast cancer.
Bibliographic Data
- Title: Diagnostic performance of mammography and ultrasound in breast cancer: a systematic review and meta-analysis
- Authors: Getu Ferenji Tadesse, Eyachew Misganew Tegaw, Ejigu Kebede Abdisa
- Journal: Journal of Ultrasound
- Year: 2023
- DOI: 10.1007/s40477-022-00755-3
Original Article:
Full text PubMed Central
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.