
Comment:
A solid, though non-systematic, review that effectively compiles preclinical evidence showing how hyperglycemia drives chemoresistance via metabolic reprogramming (the Warburg effect). Crucially, it reminds us that aggressive glycemic control is a clinically relevant intervention.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
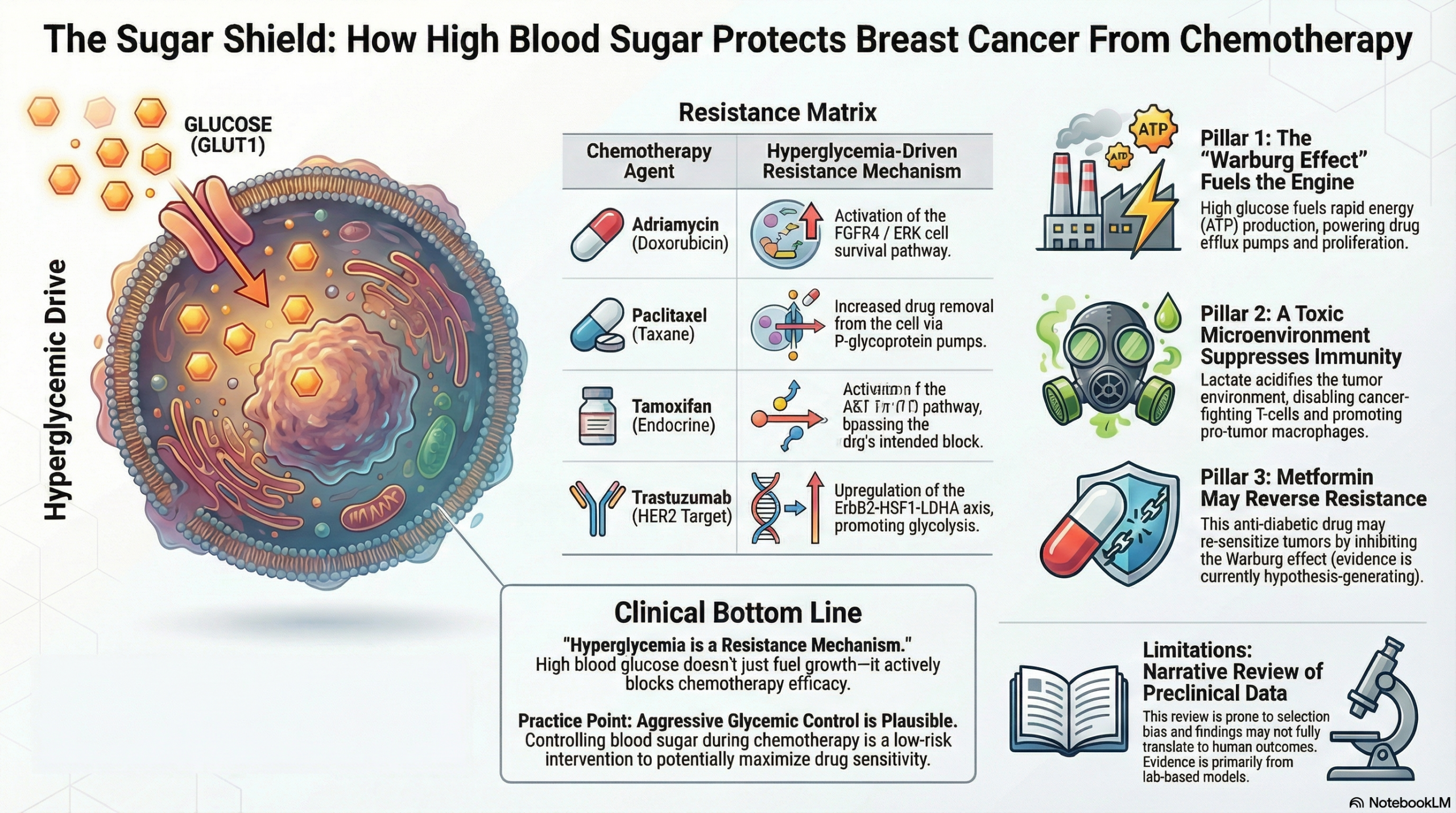
This narrative review synthesizes preclinical and clinical evidence suggesting that hyperglycemia is a significant driver of chemoresistance in breast cancer, mediated through metabolic reprogramming (the Warburg effect), activation of survival pathways (PI3K/AKT/mTOR), and alteration of the tumor microenvironment (TME). While the authors highlight the potential of antidiabetic agents like metformin to reverse this resistance, clinicians should view these recommendations as hypothesis-generating. The review lacks the rigor of a systematic search or quality assessment, meaning the conclusions are subject to selection bias and rely heavily on mechanistic data rather than high-level clinical evidence.
Key Themes & Mechanisms in Context
- Metabolic Reprogramming (The Warburg Effect):
- Tumor cells in hyperglycemic conditions upregulate glycolysis and glucose uptake via GLUT1 even in the presence of oxygen (aerobic glycolysis).
- This inefficient ATP production leads to increased lactate fermentation.
- High glucose levels stabilize GLUT1 through the USP6NL/AKT pathway, fueling proliferation and invasion.
- Mechanisms of Drug Resistance:
- The review details how hyperglycemia interferes with specific chemotherapy agents:
- Adriamycin (Doxorubicin): Resistance is linked to insulin resistance and the upregulation of the FGFR4-FRS2-ERK signaling pathway.
- Paclitaxel: Resistance is associated with lactate dehydrogenase A (LDHA) activity and drug efflux via P-glycoprotein, which is fueled by glycolytic ATP.
- Tamoxifen: In ER-positive breast cancer, hyperglycemia activates the AKT/mTOR/AMPK axis, bypassing estrogen receptor blockade.
- Trastuzumab (Herceptin): Sensitivity is inversely related to glycolytic activity; aerobic glycolysis inhibition via the ErbB2-HSF1-LDHA pathway can restore sensitivity.
- The review details how hyperglycemia interferes with specific chemotherapy agents:
- The Tumor Microenvironment (TME):
- Hyperglycemia contributes to an acidic, hypoxic, and inflammatory microenvironment.
- Lactate accumulation promotes the polarization of macrophages to the M2-like phenotype (immunosuppressive and pro-tumorigenic).
- High glucose competes with T-cells for resources, impairing anti-tumor immunity.
- Therapeutic Implications:
- Metformin: Highlighted as a key adjunct. It inhibits mitochondrial function and the mTOR pathway, potentially reversing the Warburg effect and reducing circulating estrogen.
- Current Status: Multiple clinical trials are recruiting or completed to test metformin in neoadjuvant and adjuvant settings, though results on pathological complete response (pCR) have been mixed or are still pending (Tables 1 & 2).
Assertive Critical Appraisal
- Review Methodology (Narrative vs. Systematic):
- Critique: This is a Narrative Review, not a Systematic Review. The authors do not present a defined search strategy, inclusion/exclusion criteria, or a PRISMA flow diagram.
- Impact: Without a systematic approach, the review is prone to selection bias. The authors may have preferentially selected studies that support the link between hyperglycemia and chemoresistance while omitting conflicting data. Clinicians cannot assume this represents the totality of the available evidence.
- Certainty of Evidence (GRADE Perspective):
- Rating: Low to Very Low for clinical application.
- Rationale: The majority of the mechanistic evidence cited is derived from preclinical models (cell lines like MDA-MB-231 and MCF-7, and mouse models). While biologically plausible, these findings do not always translate to human clinical outcomes. The clinical evidence discussed primarily involves retrospective associations or Phase II trials.
- Reporting Quality:
- Flaw: The review conflates different breast cancer subtypes (TNBC, ER+, HER2+) in its general discussion of hyperglycemia. While specific sections address specific drugs (e.g., Tamoxifen for ER+), the general effects of hyperglycemia on “breast cancer behavior” are often generalized, which may oversimplify the metabolic heterogeneity between subtypes.
- Publication Bias:
- The authors did not assess for publication bias. Given that negative studies regarding metabolic interventions (e.g., dietary changes or metformin) are common, the absence of this assessment further suggests the conclusions may be overly optimistic regarding the impact of glucose modulation.
Research Objective
To review the latest progress in defining the cellular mechanisms of chemotherapy resistance in hyperglycemic breast cancer patients and explore the impact of abnormal glucose metabolism on key signaling pathways and treatment response.
Study Design
Narrative Literature Review.
Setting and Participants
The review aggregates data from various preclinical (in vitro and in vivo) studies and clinical trials involving breast cancer patients with hyperglycemia or diabetes.
Bibliographic Data
- Authors: Qiu J, Zheng Q, Meng X.
- Title: Hyperglycemia and Chemoresistance in Breast Cancer: From Cellular Mechanisms to Treatment Response.
- Journal: Frontiers in Oncology.
- Year: 2021.
- DOI: 10.3389/fonc.2021.628359
Original Article:
Full text: PubMed Central
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.