
Key Information: What You Should Know Before Your Mammogram
This summary helps you learn about breast screening using a mammogram (an X-ray picture of the breast). It can help you decide if you want to have this screening. Please read this entire booklet or have someone read it with you.
- Primary Purpose: The goal of this screening is to find breast cancer early, before you can feel a lump. Finding it early may make it easier to manage.
Serious Risks:
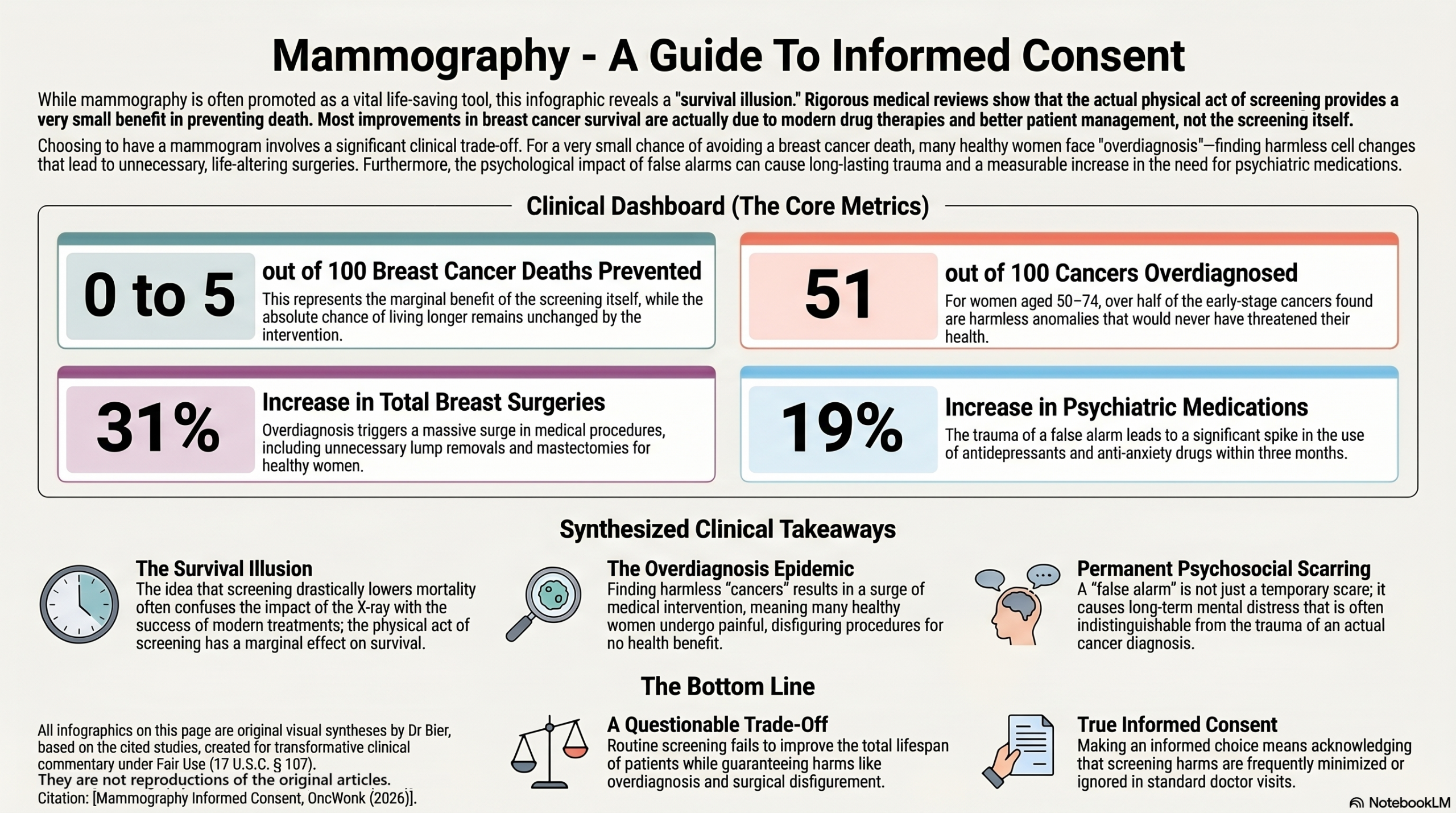
- Overdiagnosis: The X-ray test can find a cancer that would never become a threat to your health during your lifetime. Because doctors cannot tell which cancers are harmless, you may receive surgery to your breast, radiation and medications that you do not actually need.
- Radiation-Induced Cancer: The X-ray test uses radiation that can sometimes cause additional cancers. For every 100,000 women screened yearly from age 40 to 74, about 125 women will get an additional cancer caused by the radiation, meaning 99,875 out of 100,000 women will not.
Common Risks:
- False Alarms: The test may look like cancer is there when it is not. About 20 to 60 out of 100 women will have a false alarm after 10 screens, meaning 40 to 80 out of 100 women will not. This leads to extra tests and can cause worry for years.
- Pain: About 50 out of 100 women say that having a mammogram is painful, meaning the other 50 out of 100 women do not find it painful.
Your Choice: You can choose to have a mammogram, or you can choose to do self monitoring and only receive a diagnostic mammogram if you feel a change in your breast.
What is the goal of this screening?
Doctors use mammograms to take an X-ray picture of the breast. They want to find cancer at an early stage when it is small. The bottom line, or “gist”, is that they hope this will help more women avoid dying from breast cancer.
What will happen if you choose to have a mammogram?
If you decide to have a mammogram, you will have an X-ray of your breast.
- The Procedure: Your breast will be pressed between plates to take the picture.
- The Results: If the X-ray shows something that does not look normal, you may need more tests, like an ultrasound or a biopsy (taking a small piece of tissue to check for cancer).
- Follow-up: Many screening programs invite women back every 1 to 2 years.
What are the chances a mammogram will help you?
- To understand the true benefits of screening, it is important to know the difference between breast cancer-specific mortality (your chance of dying specifically from breast cancer) and overall mortality (your total life span, or chance of dying from any cause).
- Breast Cancer-Specific Survival: It is common to hear that screening drastically lowers your chances of dying from breast cancer. Although women who screen are less likely to die of breast cancer. it is unclear whether this is due to the impact of screening, or the make up of the group who attends screening, versus those who don’t. Women who volunteer for regular screening tend to be healthier overall compared to those who don’t, which is known as a ‘healthy user bias’. When we isolate the actual medical interventions, rigorous population reviews show that modern systemic therapies and improved patient management lowered breast cancer deaths by 28 out of 100, while the physical act of screening itself only lowered it by a marginal 0 to 5 out of 100.
- Total Life Span (Overall Survival): The fundamental goal of any medical screening is to extend your overall life. Decades of the highest-quality medical trials demonstrate that routine mammography fails to improve overall survival. This means your absolute chance of living longer is exactly the same whether you participate in a screening program or not. This occurs because the true reduction in breast cancer deaths is so small that it cannot significantly alter your total lifespan, and the physical harms of overdiagnosis can introduce new, competing health risks.
Risks and Benefits by Age Category
Based on clinical data, the following table summarizes the risks and benefits for different age groups.
|
Age Group |
Primary Benefits |
Key Risks and Harms |
|
40 to 49 years |
No Clear Difference: The most rigorous records show that screening does not make a statistically significant difference in breast cancer deaths for women under 50 (a ratio of 0.94). |
Reduced Accuracy: Mammograms are less accurate for this group because younger women often have more dense breast tissue. Higher Radiation Risk: Women who start screening earlier receive more radiation over their lifetime. |
|
50 to 69 years |
Lives Saved: Over 10 years, if 2,000 women are screened, 1 woman avoids dying of breast cancer. This means 1,999 out of 2,000 women will not avoid death because of the screening. |
Overdiagnosis: For every 1 death avoided, between 10 and 14 healthy women are unnecessarily treated for harmless cell changes. False Alarms: Over 10 years, 20 to 60 out of 100 women will have at least one false alarm. |
|
70 to 74 years |
Early Detection: Screening continues to find early-stage cancers. |
Higher Overdiagnosis: The rate of overdiagnosis increases as women get older. In one review, 51 out of 100 early cancers found in women aged 50 to 74 were overdiagnosed. |
|
75 years and older |
None Proven: No rigorous randomized records have ever included women aged 75 or older. |
Burdens: In one review of screened women with an average age of 81, 17 out of 100 experienced significant burdens from the mammogram. Furthermore, official guidelines do not recommend screening for women older than 74 because of insufficient evidence. The most important harm is overdiagnosis, where women face the costs and physical toll of treatments (like surgery or radiation) that offer no health benefit and can even cause new fatal conditions. |
How can mammograms hurt you?
It is important to understand the bad things that can happen.
Unnecessary Diagnosis (Overdiagnosis):
This is a major harm. For every 1 woman who avoids dying from cancer because of screening, records show that between 10 and 14 other healthy women will be told they have a cancer that was never a threat to them.
Surgical Harm:
Overdiagnosis leads directly to extra surgery. Data shows that participating in a screening program increases a woman’s risk of having breast surgery (lump removals and breast removals combined) by 31%. Furthermore, even though screening aims to catch cancers early, the data shows it actually increases a woman’s risk of receiving a complete breast removal (mastectomy) by 20%.
Missing Cancer (False Negatives):
A mammogram can miss a cancer that is actually there. In large population screening studies, mammograms successfully find 81 out of 100 cancers, meaning they completely miss 19 out of 100 cancers.
Psychological Harm: False Alarms and ‘Dense Breast’ Letters:
Simply receiving a routine letter notifying you that you have “dense breasts” can cause unintended emotional harm. High-quality trials show these notifications significantly increase feelings of anxiety, confusion, and worry about getting breast cancer. Even when the letters are written simply, women often report that they do not feel more informed or capable of making decisions about their breast health. Instead, the letters create uncertainty, particularly for women with lower educational backgrounds or language barriers. This widespread confusion leads many women to seek out extra tests, like ultrasounds, which directly exposes them to the high false alarm risks detailed below.
The test may indicate you have cancer when you do not. About 20% to 60% of women will experience at least one false alarm after 10 rounds of screening mammograms.
The psychological burden of a false alarm is not just a brief scare. The psychosocial consequences are “just as great” as an actual breast cancer diagnosis at the six-month mark, and even at three years, their distress remains significantly worse than women with normal findings.
The emotional toll can last for over a decade. Even 12 to 14 years after a false alarm, women report a statistically significant negative impact on their existential values (a 0.61 worse score) compared to women who had normal results. Furthermore, women who have experienced a false positive have 27% higher odds of feeling that everything is an effort, 27% higher odds of feeling worthless, 23% higher odds of feeling restless, and 18% higher odds of feeling sad.
Experiencing a false positive increases the likelihood that a commercially insured woman will initiate prescription antidepressants or anti-anxiety medications by 19% within three months of the mammogram. Women with a history of false alarms also have 28% higher odds of seeking care from a mental health professional.
Highest Risk Groups: The risk of needing psychiatric medication increases drastically depending on the follow-up required: there is a 68% increased risk of initiating medication if the false alarm leads to a biopsy, a 37% increased risk if it requires multiple follow-up tests, and a 21% increased risk if it takes more than a week to be resolved. Additionally, commercially insured women aged 40 to 49 face a 33% increased risk of initiating anxiety or depression medications. Regarding long-term emotional symptoms, women under 50 have 65% higher odds of feeling that everything is an effort, and African American women have 92% higher odds of feeling restless compared to white women.
Risks and Benefits by Breast Type
Risks and Benefits by Breast Type
The following table compares the risks and benefits for women with different breast types.
| Category | Primary Benefits | Key Risks and Harms |
|
Normal |
Cancer Detection: Finds about 81 out of 100 cancers, meaning 19 out of 100 are not found early. | Surgical Harm: Between 10 and 14 out of 2,000 healthy women will receive unnecessary breast surgery or radiation for harmless cancer over a 10 year screening period. |
| Large Breasts |
Benefit Balance: For women with large breasts who get screened every year, the X-ray test prevents 4 breast cancer deaths, but it causes 1 additional cancer from the radiation. |
Higher Radiation Risk: These women have about a 2.3 times higher risk of a new cancer from radiation (266 per 100,000) than average breasts (113 per 100,000). Extra Views: About 8 out of 100 women need extra X-ray pictures to complete the test, meaning 92 out of 100 do not. |
|
Dense
|
Improved Detection: For women with dense breasts, ultrasound finds significantly more cancers than mammograms alone. In a direct comparison, ultrasound successfully found about 85 out of 100 cancers in dense breasts, whereas mammograms found only about 62 out of 100. Accuracy in Extreme Density: For women with “extremely dense” breasts, mammograms missed more than half of the cancers present (finding only 44 out of 100), while ultrasound maintained its high accuracy (finding 84 out of 100). |
More False Alarms: Because ultrasound is so sensitive, it is less specific than a mammogram. When ultrasound is added to a mammography screening routine, the false alarm rate increases 2.5 times (jumping from 22 false alarms per 1,000 women with mammography alone to 55 per 1,000 women). This means 33 additional healthy women out of every 1,000 will be told they might have cancer. This leads directly to more healthy women receiving extra tests and benign biopsies they did not actually need. This can cause considerable and sustained psychological distress and sleep problems that last for years, even after the biopsy proves they are cancer-free. Unnecessary Biopsies: Because of the cascade of extra tests and benign biopsies triggered by these false alarms, ultrasound is not recommended for everyone. It represents a specific trade-off for women with dense breasts who are willing to accept a much higher risk of false alarms to improve their cancer detection.
|
What are your other options?
You do not have to have a mammogram.
- Do Nothing: You can choose to not be screened at all. You would only receive a diagnostic mammogram if you feel a lump or notice a change.
- Other Tests: For women with dense breasts, an ultrasound might be used, but as noted above, it detects more cancers and causes more false positive results than a mammogram when used alone.
Glossary of Terms
- Biopsy: A small medical procedure to take a piece of tissue from the breast to see if cancer is present.
- Dense Breasts: Breasts that have more gland tissue and less fat tissue, which makes it harder for X-rays to see through.
- False Alarm (False Positive): When the test looks like a problem is there, but further checks prove there is no problem.
- Overdiagnosis: Finding a cancer that would never have grown or caused you to get sick if it had never been found.
- Radiation-Induced Cancer: A rare risk where the X-ray radiation itself causes an additional cancer to form years later.
- Ultrasound: A test that uses sound waves to create a picture of the inside of the breast.
Sources
Argov, E. J., Rodriguez, C. B., Agovino, M., Wei, Y., Shelton, R. C., Kukafka, R., Schmitt, K. M., Desperito, E., Terry, M. B., & Tehranifar, P. (2022). Breast cancer worry, uncertainty, and perceived risk following breast density notification in a longitudinal mammography screening cohort. Breast Cancer Research, 24(1), 95. https://doi.org/10.1186/s13058-022-01584-2.
Autier, P., Boniol, M., Koechlin, A., Pizot, C., & Boniol, M. (2017). Effectiveness of and overdiagnosis from mammography screening in the Netherlands: population based study. BMJ, 359, j5224. https://doi.org/10.1136/bmj.j5224
Autier, P., Jørgensen, K. J., Smans, M., & Støvring, H. (2024). Effect of screening mammography on the risk of breast cancer deaths and of all-cause deaths: a systematic review with meta-analysis of cohort studies. Journal of Clinical Epidemiology, 172, 111426. https://doi.org/10.1016/j.jclinepi.2024.11.1426
Bolejko, A., Hagell, P., Wann-Hansson, C., & Zackrisson, S. (2015). Prevalence, long-term development, and predictors of psychosocial consequences of false-positive mammography among women attending population-based screening. Cancer Epidemiology, Biomarkers & Prevention, 24(9), 1388–1397. https://doi.org/10.1158/1055-9965.EPI-15-0060
Brodersen, J., & Siersma, V. D. (2013). Long-term psychosocial consequences of false-positive screening mammography. Annals of Family Medicine, 11(2), 106–115. https://doi.org/10.1370/afm.1466
Dolan, H., McCaffery, K., Houssami, N., Cvejic, E., Brennan, M., Hersch, J., Dorrington, M., Verde, A., Vaccaro, L., & Nickel, B. (2022). Australian Women’s Intentions and Psychological Outcomes Related to Breast Density Notification and Information: A Randomized Clinical Trial. JAMA Network Open, 5(6), e2216784. https://doi.org/10.1001/jamanetworkopen.2022.16784.
Duffy, S. W., Vulkan, D., Cuckle, H., Parmar, D., Sheikh, S., Smith, R. A., Evans, A., Blyuss, O., Johns, L., Ellis, I. O., Myles, J., Sasieni, P. D., & Moss, S. M. (2020). Effect of mammographic screening from age 40 years on breast cancer mortality (UK Age trial): final results of a randomised, controlled trial. The Lancet Oncology, 21(9), 1165–1172. https://doi.org/10.1016/S1470-2045(20)30398-3
Gøtzsche, P. C., & Jørgensen, K. J. (2013). Screening for breast cancer with mammography. Cochrane Database of Systematic Reviews, (6), Article CD001877. https://doi.org/10.1002/14651858.CD001877.pub5
Gram, E. G., Siersma, V., & Brodersen, J. B. (2023). Long-term psychosocial consequences of false-positive screening mammography: a cohort study with follow-up of 12–14 years in Denmark. BMJ Open, 13(4), e072188. https://doi.org/10.1136/bmjopen-2023-072188
Jatoi, I., Zhu, K., Shah, M., & Lawrence, W. (2006). Psychological distress in U.S. women who have experienced false-positive mammograms. Breast Cancer Research and Treatment, 100(2), 191–200. https://doi.org/10.1007/s10549-006-9236-6
Kowalski, A. E. (2021). Mammograms and mortality: How has the evidence evolved? Journal of Economic Perspectives, 35(2), 119–140. https://doi.org/10.1257/jep.35.2.119
Miglioretti, D. L., Lange, J., van den Broek, J. J., Lee, C. I., van Ravesteyn, N. T., Ritley, D., Kerlikowske, K., Fenton, J. J., Melnikow, J., de Koning, H. J., & Hubbard, R. A. (2016). Radiation-induced breast cancer incidence and mortality from digital mammography screening: a modeling study. Annals of Internal Medicine, 164(4), 205–214. https://doi.org/10.7326/M15-1241
Moss, S. M., Wale, C., Smith, R., Evans, A., Cuckle, H., & Duffy, S. W. (2015). Effect of mammographic screening from age 40 years on breast cancer mortality in the UK Age trial at 17 years’ follow-up: a randomised controlled trial. The Lancet Oncology, 16(9), 1123–1132. https://doi.org/10.1016/S1470-2045(15)00128-X
Nickel, B., Copp, T., Brennan, M., Farber, R., McCaffery, K., & Houssami, N. (2021). The Impact of Breast Density Information or Notification on Women’s Cognitive, Psychological, and Behavioral Outcomes: A Systematic Review. JNCI: Journal of the National Cancer Institute, 113(10), 1299–1330. https://doi.org/10.1093/jnci/djab016.
Nickel, B., Ormiston-Smith, N., Cvejic, E., Isautier, J., Hammerton, L., Baker, K., Legerton, P., Vardon, P., McInally, Z., Robertson, S., McCaffery, K., & Houssami, N. (2025). Impact of population based breast density notification: multisite parallel arm randomised controlled trial in BreastScreen. BMJ, 391, e083649. https://doi.org/10.1136/bmj-2024-083649.
Rehman, H., Ahmad, I., Rashid, S., Mukhtar, M., Khan, A. A., & Khaliq, H. (2025). Comparison of diagnostic accuracy of ultrasound and mammography in detecting breast cancer in radiographically dense breasts. Cureus, 17(9), e92637. https://doi.org/10.7759/cureus.92637
Segel, J. E., Balkrishnan, R., & Hirth, R. A. (2017). The effect of false-positive mammograms on antidepressant and anxiolytic initiation. Medical Care, 55(8), 752–758. https://doi.org/10.1097/MLR.0000000000000752
Tadesse, G. F., Tegaw, E. M., & Abdisa, E. K. (2023). Diagnostic performance of mammography and ultrasound in breast cancer: a systematic review and meta-analysis. Journal of Ultrasound, 26(3), 355–367. https://doi.org/10.1007/s40477-022-00755-3
Wang, J., Zheng, S., Ding, L., Liang, X., Wang, Y., Greuter, M. J. W., de Bock, G. H., & Lu, W. (2020). Is ultrasound an accurate alternative for mammography in breast cancer screening in an Asian population? A meta-analysis. Diagnostics, 10(11), 985. https://doi.org/10.3390/diagnostics10110985
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.