
Comment:
If you’ve been reading any of my reviews, you know I always focus on Overall Survival as the most important metric, and this study does just that, and shows a shockingly high risk of death for those who use CAM, whether alone or with conventional treatment. The headline of the study is extremely concerning, however there are some very significant core issues related to the observational nature of the study, and the definitions they used that renders the findings to be highly suspect.
The central issue in this paper is the assumption that the choice to use complementary and alternative medicine (CAM) drove the observed survival deficits, rather than the glaring structural reality of the difference in the patients’ ages.
The cohorts are demographically distinct. Patients utilizing a combination of CAM and traditional therapies are significantly younger (median age 54) than those receiving traditional therapy alone (median age 62) or no treatment (median age 67). We must apply a biological plausibility filter: younger breast cancer patients inherently face an increased risk of aggressive, fast-growing malignancies. General oncology data consistently shows that younger women have up to a 20% rate of Triple-Negative disease and a 23% rate of HER2-positive disease—rates that are drastically higher than the ~10% and ~13% respective averages seen in older populations.
The CAM group with a median age of 54 also certainly contains far more pre-menopausal women than the traditional therapy alone group at median age of 62. The Interquartile Range (IQR) for the combination group is 44-63 years, which means the middle 50% of the patients were between 44 and 63. That means 25% of them were under 44 years old! Compare that to an IQR of 52-71 for the traditional group.
So it’s not just younger age, but menopausal status that increases high risk phenotypes present in the CAM groups:
-
Triple-Negative Breast Cancer (TNBC): Research consistently shows that pre-menopausal women have a significantly higher prevalence of TNBC—the most aggressive subtype. In women under 40, the rate is approximately 20–25%, whereas in post-menopausal women, it drops to roughly 10–12%.
-
HER2 Enrichment: Pre-menopausal status is a known risk factor for HER2-positive disease. Younger patients have a 23% rate of HER2 amplification, compared to just 13–15% in older populations.
-
Proliferation Rates (Ki-67): Tumors in pre-menopausal women generally exhibit higher Ki-67 scores (a marker of cell proliferation), often exceeding 30%, indicating a much faster doubling time than the indolent, luminal A-type cancers typically found in the 62-year-old traditional cohort.
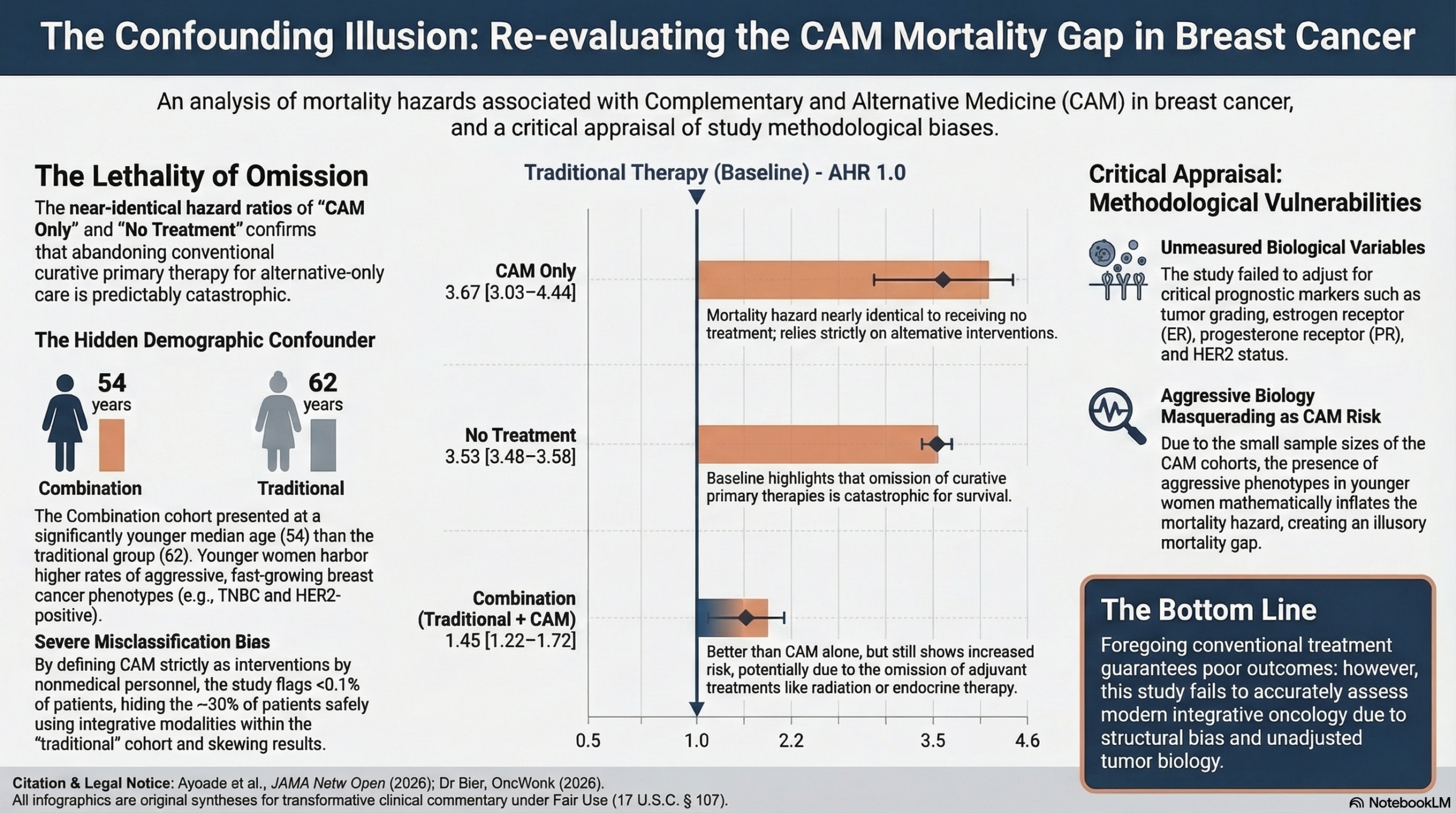
By failing to adjust their statistical models for ER/PR and HER2 status, the authors allowed this aggressive tumor biology to act as a hidden variable. In exceptionally small cohorts like the CAM-only (n=273) and combination (n=568) groups which account for under 0.04% of the study population, a higher concentration of younger women with aggressive phenotypes will mathematically guarantee a wider mortality gap, creating an illusory hazard ratio (HR 3.67 and 1.45). The definitive takeaway is that while the omission of traditional curative therapy is undisputedly dangerous, this study primarily documents the lethal nature of young-onset breast cancer, versus the impact of doing CAM therapies.
Another crucial issue for the accuracy of the results is the misclassification of CAM users. You have to approach observational registries with extreme caution when the fundamental variable being studied is structurally misclassified. The methodology of this paper defines complementary and alternative medicine strictly as “treatment administered by nonmedical personnel,” successfully flagging less than 0.04% of the total study population as CAM users. Since we know that up to 30% of breast cancer patients utilize some form of integrative therapy, this study clearly suffers from massive misclassification bias. The vast majority of patients safely utilizing evidence-based natural compounds—often under the guidance of licensed integrative physicians—are actively hidden within the “traditional therapy” cohort because their interventions are not coded as “nonmedical”, or they are simply not reporting their use. Consequently, the tiny fraction of patients actually captured in the combination and CAM-only arms do not represent typical integrative oncology; they represent a highly specific subset whose alternative choices were explicitly flagged in a conventional hospital registry. By comparing this distinct, unrepresentative fraction against a “traditional” cohort that secretly contains hundreds of thousands of successful integrative patients, the study mathematically inflates the mortality hazard of the alternative label. This creates a structural illusion that obscures the true biological impact of the interventions themselves.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This cohort study shows a strong association between the use of complementary and alternative medicine (CAM) as a replacement for, or in partial combination with, traditional therapies and an increased risk of mortality in patients with breast cancer. While these findings powerfully highlight the dangers of omitting conventional oncologic care, it is vital to remember that this is an observational study; it cannot definitively prove causation due to the high risk of unmeasured confounding variables.
Results in Context
- Main Results: Compared with patients treated with traditional therapies, those treated with CAM alone had the highest risk for mortality, demonstrating an adjusted hazard ratio (AHR) of 3.67 (95% CI, 3.03-4.44). Patients who received no treatment whatsoever had a similarly poor outcome with an AHR of 3.53 (95% CI, 3.48-3.58). The combination of traditional therapies and CAM was also associated with a higher mortality compared with being treated exclusively with traditional therapy (AHR, 1.45; 95% CI, 1.22-1.72).
- Definitions: An adjusted hazard ratio of 3.67 means that, after accounting for measured variables like age and clinical stage, the risk of death at any given time for the CAM-only group was 3.67 times higher than for the traditional therapy group.
- Participants: The sample included 2,157,219 female patients diagnosed with breast cancer. A total of 2,106,665 patients (97.6%) received traditional therapy, 49,713 (2.3%) received no treatment, 568 (<0.1%) received combination therapy, and 273 (<0.1%) received CAM alone.
Assertive Critical Appraisal
- Limitations & Bias (STROBE Framework): The NCDB defines alternative therapy strictly as treatment administered by nonmedical personnel. This narrow definition likely introduces massive misclassification bias, capturing only a fraction of patients using CAM. The authors acknowledge that other studies estimate CAM use in breast cancer closer to 30%, meaning the vast majority of integrative therapy users are likely hidden within the “traditional therapy” cohort.
- Reporting Quality Assessment (STROBE/RECORD): The authors adjust for several confounders including age, race, Charlson Comorbidity index, and clinical tumor stage. However, the study fails to adjust for specific tumor biology, such as estrogen receptor (ER), progesterone receptor (PR), or human epidermal growth factor receptor 2 (HER2) status in their Cox model. Omission of tumor grading and receptor status when evaluating breast cancer survival is a major methodological vulnerability.
- Demographic Disparities: There are striking age differences between the cohorts. The combination group was the youngest (median age 54), the traditional therapy group had a median age of 62, and the no-treatment group was the oldest (median age 67). Clinically, this implies younger patients may be seeking CAM due to a stronger desire for holistic control or deeper fears regarding the long-term toxicities of conventional treatments. Conversely, older patients in the “no treatment” arm may reflect a high frailty burden or a conscious shift toward palliative care goals.
- Unmeasured Confounding: The sample sizes for the CAM-only (n=273) and Combination (n=568) cohorts are exceedingly small relative to the overall population. Because the study lacks adjustment for specific, aggressive tumor biology like Triple-Negative or HER2-positive status, unmeasured confounding is a critical threat. A slight overrepresentation of these highly aggressive phenotypes in these tiny cohorts could drastically skew the survival outcomes, creating a misleadingly large mortality gap that is driven by tumor biology rather than the choice of CAM.
- Clinical Context vs. Statistical Magnitude: The reported Hazard Ratios tell a distinct clinical story regarding the omission of care. The HR for the CAM-only group (3.67) is mathematically nearly identical to the “no treatment” group (3.53). This strongly implies that relying solely on CAM equates to the total omission of primary curative treatments like surgery and systemic chemotherapy. Conversely, the combination group (HR 1.45) showed lower survival than traditional therapy, which the authors correlate with a higher likelihood of omitting adjuvant treatments like radiation and endocrine therapy. Skipping these adjuvant therapies increases the risk of recurrence over a longer time horizon, which mathematically aligns with the moderate mortality increase (HR 1.45) seen in the combination cohort compared to the catastrophic mortality seen when primary therapies are skipped entirely.
- Applicability: The findings are highly relevant to general oncology practice, as the NCDB captures roughly 70% of newly diagnosed cancers in the US. However, the results specifically apply to patients who decline conventional care in favor of alternative practitioners, rather than those integrating safe supplements or mind-body practices as an adjunct to full standard-of-care.
Research Objective
To describe the association of complementary and alternative medicine (CAM) with survival in female patients with breast cancer.
Study Design
This was a retrospective cohort study.
Setting and Participants
The study analyzed data from the National Cancer Database (NCDB). It included 2,157,219 female patients diagnosed with breast cancer between 2011 and 2021.
Bibliographic Data
- Title: Use of Complementary and Alternative Medicine in the Management of Breast Cancer
- Authors: Oluwaseun F. Ayoade, MD, MSHA; Giorgio Caturegli, MD; Maureen E. Canavan, PhD, MPH; Benjamin J. Resio, MD; Elizabeth R. Berger, MD, MS; Daniel J. Boffa, MD, MBA
- Journal: JAMA Network Open
- Year: 2026
- DOI: 10.1001/jamanetworkopen.2026.0337
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.