
Comment:
A screening tool can only be as effective as the patient’s adherence to it. This NordICC study has been widely misrepresented as evidence of colonoscopy’s limited impact, yet that narrative relies on an intention-to-screen analysis that reflects an invitation to a procedure rather than the procedure itself.
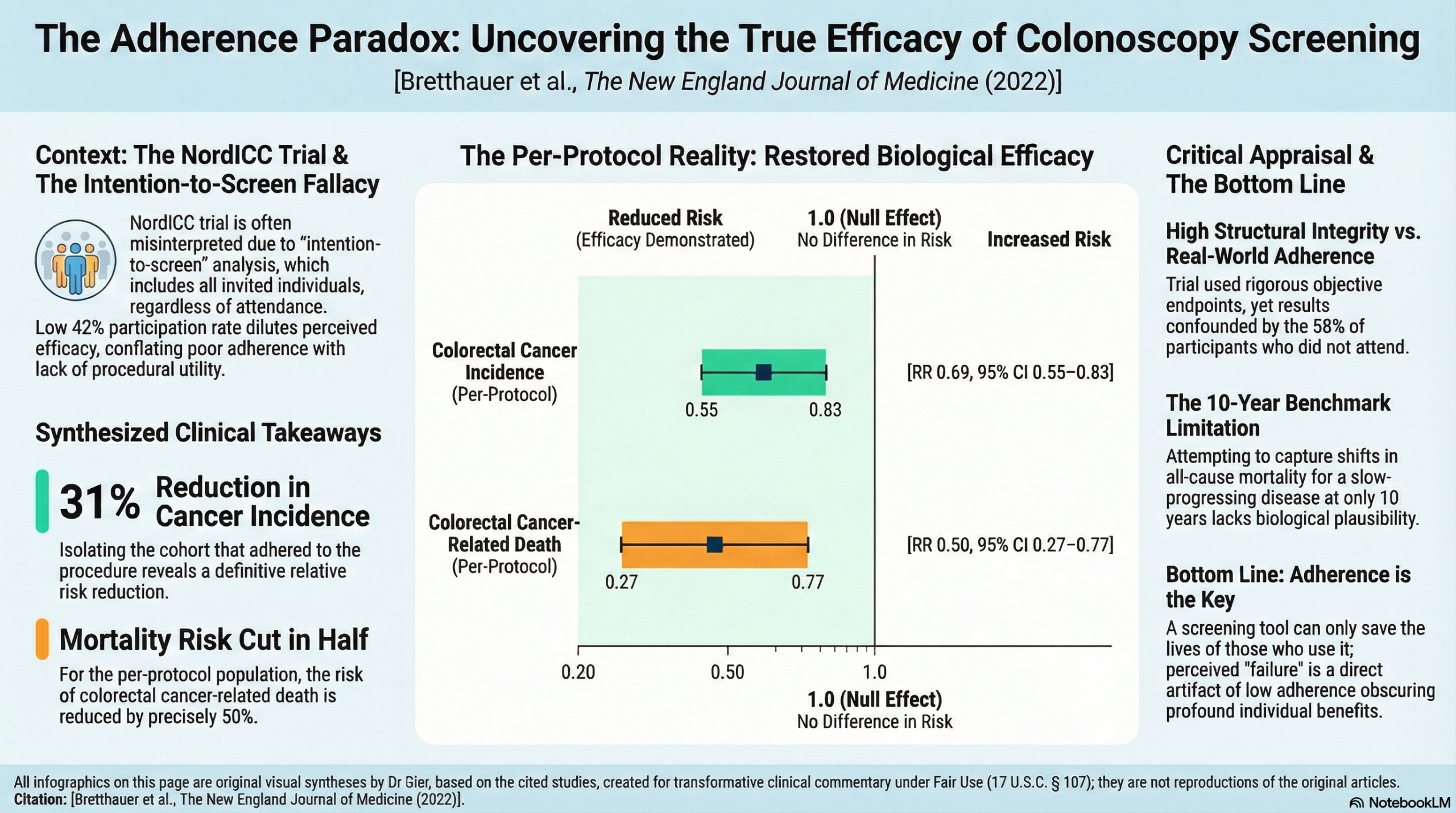
The NordICC results are a perfect example of a “survival paradox”: the intention-to-screen analysis shows a modest gain. however the reported modest 18% reduction in cancer incidence is a statistical mirage fueled by the 58% of participants who never actually showed up. When we look at the per-protocol data, the 42% who actually did the screening, the hazard ratio for colorectal cancer death drops by a staggering 50%. Shockingly the people who go the gym to exercise have better outcomes compared to those who just got mailed an advertising flyer. There’s nothing wrong with evaluating the impact of a program, whether it’s invitation to screening or a free gym membership. And we have to make a distinction between the evaluation of the results of a program offering, and the results seen by people who actually participate in it.
Another issue with this study is the lack of change in overall survival in the group that did screen. This is likely due to the slow physiological progression of colorectal cancer and the premature demand for overall survival (OS) data at the 10-year mark. While critics point to the lack of a significant OS signal in this randomized trial, we should use a biological plausibility filter: it is mathematically impossible to move the needle on all-cause mortality in a healthy population over a decade when the absolute death rate from the target disease is just 0.3%. I continue to focus on OS as the ultimate metric, but only when the study is powered and timed to see it. At 10 years, we are seeing the “lead-time” phase of a slow-growing disease. The takeaway is that the 50% reduction in cancer-related death in the screened group confirms the efficacy of the tool, and any perceived failure to impact OS is a statistical non-event caused by insufficient duration and small numbers.
Summary:
Clinical Bottom Line
This large-scale, pragmatic randomized trial (NordICC) provides high-quality evidence that an invitation to a single screening colonoscopy reduces the 10-year incidence of colorectal cancer (CRC) by 18%. However, in this 10-year follow-up period, the intervention did not significantly reduce CRC-related mortality or all-cause mortality in the “intention-to-screen” analysis. While the “per-protocol” analysis (estimating the effect if everyone invited had actually attended) suggests more substantial benefits—up to a 31% reduction in CRC incidence and a 50% reduction in CRC death—these must be viewed with caution as they are adjusted estimates rather than direct trial results. Clinicians should note the relatively low participation rate (42%), which reflects real-world challenges in population-based screening.
Results in Context
Primary Outcomes
- Colorectal Cancer Incidence: The 10-year risk was 0.98% in the invited group vs. 1.20% in the usual-care group. The risk ratio (RR) was 0.82 (95% CI, 0.70 to 0.93), representing an 18% relative risk reduction.
- Colorectal Cancer-Related Death: The 10-year risk was 0.28% in the invited group vs. 0.31% in the usual-care group. The RR was 0.90 (95% CI, 0.64 to 1.16), which was not statistically significant as the confidence interval crosses 1.0.
Key Secondary & Specialized Outcomes
- Death from Any Cause: No significant difference was found between groups (11.03% in the invited group vs. 11.04% in the usual-care group; RR 0.99).
- Number Needed to Invite (NNI): To prevent one case of CRC, 455 people (95% CI, 270 to 1429) would need to be invited to undergo screening.
- Cancer Staging: There was no significant difference in the detection of late-stage (Dukes’ C or D) cancers between the invited (0.40%) and usual-care (0.50%) groups.
Harms and Adverse Events
- Major Bleeding: Occurred in 15 participants (0.13% of those screened) following polyp removal; all were treated endoscopically without further intervention.
- Perforations: There were no perforations or screening-related deaths reported within 30 days of the procedure in the analyzed cohort.
Assertive Critical Appraisal
Risk of Bias (RoB 2)
Judgment: Low Risk. The trial used a robust, computer-generated randomization process stratified by age, sex, and municipality. While it was unblinded (inherent to screening trials), the primary endpoints were objectively verified through national cancer and death registries, which minimizes detection bias.
Subgroup Analyses: Geographic Variance
The screening benefit appeared more pronounced in Norway (per-protocol RR 0.55) compared to Poland (per-protocol RR 0.85). However, the authors correctly note that confidence intervals were overlapping and event rates were small, meaning these country-specific differences should be viewed as hypothesis-generating rather than definitive.
Reporting Quality Assessment (CONSORT)
The reporting quality is high. The study clearly describes randomization, provides a detailed “No. at Risk” breakdown in its figures, and includes a comprehensive table (Table 1) of participant characteristics and screening performance metrics.
Applicability
The results are highly relevant to European populations and provide a “real-world” estimate of what a population-based invitation program can achieve. However, the 10-year follow-up may be too short to capture the full mortality benefit of colonoscopy, as CRC is a slow-progressing disease. The low participation rate (42%) also means the results may not apply to systems with higher adherence or different cultural attitudes toward invasive screening.
Research Objective
To investigate the effect of a single population-based colonoscopy screening invitation on the risks of colorectal cancer and related death at 10 years.
Study Design
A pragmatic, randomized, controlled trial using a 1:2 ratio (invitation to screening vs. usual care). The trial utilized a “randomize, then consent” design where participants were identified via population registries and only those in the invited group who chose to participate provided consent.
Setting and Participants
- Setting: Poland, Norway, and Sweden (data from the Netherlands were excluded due to legal/GDPR constraints).
- Participants: 84,585 healthy men and women aged 55 to 64 years.
- Groups: 28,220 in the invited group and 56,365 in the usual-care group.
Bibliographic Data
- Title: Effect of Colonoscopy Screening on Risks of Colorectal Cancer and Related Death
- Authors: M. Bretthauer, M. Løberg, P. Wieszczy, et al. (NordICC Study Group)
- Journal: The New England Journal of Medicine
- Year: 2022
- DOI: 10.1056/NEJMoa2208375
Would you like me to compare these findings to existing data on fecal immunochemical testing (FIT) or flexible sigmoidoscopy mentioned in the discussion?
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.