
Comment:
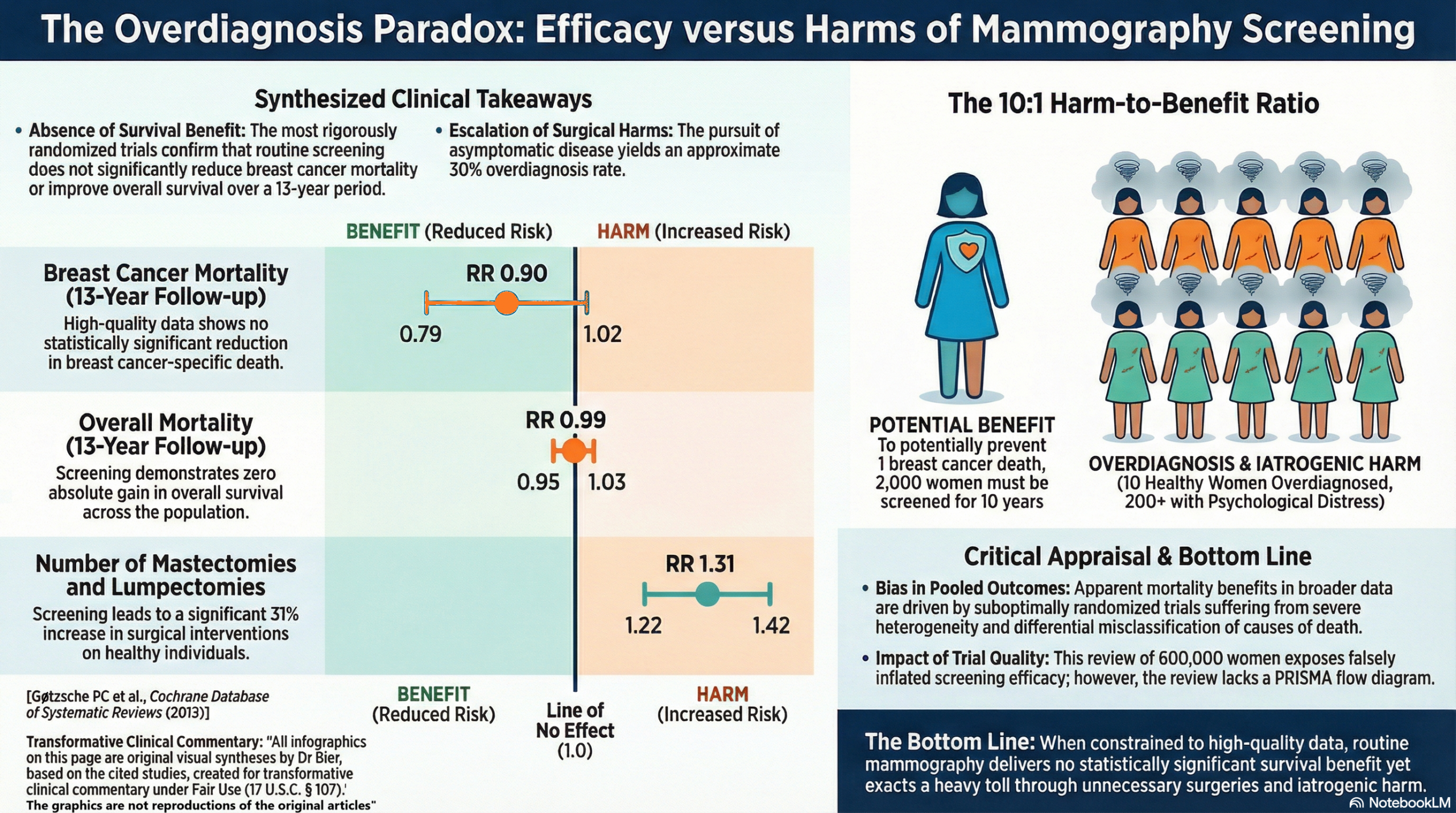
The traditional clinical focus on “saving lives from breast cancer” ignores the underlying reality that “detecting a tumor earlier” does not equate to “lengthening that patient’s life.” This Cochrane review of 600,000 women published in 2013 deconstructs the evidence to reveal that while biased, suboptimally randomized trials suggest a benefit, the three adequately randomized trials showed no statistically significant reduction in breast cancer mortality (RR 0.90, 95% CI 0.79 to 1.02). We should recognize that even this marginal signal is likely an artifact of differential misclassification, where the act of screening ensures deaths are coded as cancer-related in the control group while being ‘cleansed’ from the screening cohorts. To potentially prevent a single breast cancer death, 2,000 women must be screened for 10 years. In that same decade, 10 healthy women will be overdiagnosed and channeled into unnecessary mastectomies and radiation, while over 200 will experience years of psychological distress from false positives.
It highlights the “Overdiagnosis Paradox”: for every woman who avoids a cancer death through screening, ten others are “fixed” for a disease they never truly had, or at least would never have manifested in their lifetime. This iatrogenic legacy results in a 31% increase in total surgical interventions and a 20% increase in mastectomies, as clinicians chase indolent lesions that would never have surfaced naturally. Prioritizing hard clinical endpoints requires us to acknowledge that the 10:1 harm-to-benefit ratio is a measurable price of risk paid for zero absolute gain in overall survival.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This systematic review provides compelling evidence that while breast cancer screening with mammography may offer a slight reduction in breast cancer-specific mortality in heavily biased studies, the most rigorously conducted trials demonstrate no statistically significant benefit in overall survival or breast cancer mortality. Furthermore, screening introduces substantial risks, notably a 30% rate of overdiagnosis, which directly leads to unnecessary mastectomies, radiation therapy, and significant psychological distress for healthy women.
Results
Summary of Results
- Breast Cancer Mortality: In the three adequately randomized trials, there was no statistically significant reduction in breast cancer mortality after 13 years of follow-up (Relative Risk [RR] 0.90, 95% Confidence Interval [CI] 0.79 to 1.02). An RR of 0.90 indicates a 10% reduction in the risk of death, but because the confidence interval crosses 1.0, the result is not statistically significant and could be due to chance.
- Overall Survival and Cancer Mortality: The highest quality trials found no effect of screening on total cancer mortality after 10 years (RR 1.02, 95% CI 0.95 to 1.10). Most importantly, there was no benefit to all-cause mortality (overall survival) after 13 years (RR 0.99, 95% CI 0.95 to 1.03).
- Harms and Overtreatment: Screening led to a massive increase in surgical interventions. The combined number of lumpectomies and mastectomies was significantly higher in the screened groups (RR 1.31, 95% CI 1.22 to 1.42), as was the rate of mastectomies alone (RR 1.20, 95% CI 1.08 to 1.32). The use of radiotherapy was similarly increased among screened women.
Assertive Critical Appraisal
Certainty of Evidence (GRADE Framework) The certainty of evidence for the lack of an overall survival benefit is Moderate to High, driven by the large, adequately randomized trials. However, the certainty of evidence for any breast cancer-specific mortality benefit is Low. The reviewers explicitly downgrade the reliability of breast cancer mortality as an endpoint because it was found to be biased in favour of screening, largely due to the differential misclassification of the cause of death.
Heterogeneity The review identified severe heterogeneity (the percentage of variation across studies due to real differences rather than just chance) when comparing trial quality. The four suboptimally randomized trials showed a highly significant reduction in breast cancer mortality (RR 0.75, 95% CI 0.67 to 0.83), while the adequately randomized trials showed no significant effect. This drastic variation indicates that methodological flaws are driving the positive results seen in the poorly conducted studies, and pooled averages should be interpreted with extreme caution.
Publication Bias The authors utilized a broad search strategy spanning PubMed and the World Health Organization’s International Clinical Trials Registry Platform, with no language restrictions. While the authors did not explicitly report on funnel plots or Egger’s test in this summary, it is a well-known contextual truth that publication bias is a common threat that can lead to an overestimation of treatment effects.
Risk of Bias in Included Studies The authors rigorously evaluated the trials and excluded one entirely because its randomization failed to produce comparable groups. Of the remaining trials, four were deemed “suboptimal” due to severe biases, including unblinded cause-of-death assessments and baseline imbalances. These biases heavily favoured the screening cohorts, artificially inflating the perceived benefits of mammography.
Special Consideration for Pooled Results When combining all seven trials, the review notes a statistically significant reduction in breast cancer mortality (RR 0.81, 95% CI 0.74 to 0.87). It is important to note that while the overall pooled result is statistically significant, this conclusion is derived from a collection of smaller or biased studies, the majority of the high-quality ones which did not find a significant effect on their own. This scenario often occurs when individual studies are underpowered (too small) to detect a modest but real treatment effect. By combining their data, the meta-analysis increases the overall statistical power, which can reveal a consistent trend that was not apparent in the smaller studies. However, this finding should be interpreted with caution. It is crucial to assess for significant heterogeneity (differences between studies) and the potential for publication bias (the possibility that unpublished negative studies are missing), as either of these factors could lead to a misleading pooled result.
Reporting Quality Assessment (PRISMA) The review clearly outlines its methodology, search parameters, and inclusion criteria. However, I must explicitly flag that the review does not include a PRISMA flow diagram showing the study selection process in the provided text. This omission reduces the immediate transparency and reproducibility of the review’s attrition process for the clinician reading the summary.
Study Details
- Research Objective: To assess the effect of screening for breast cancer with mammography on mortality and morbidity (comparing screened women against non-screened women).
- Study Design: Systematic review and meta-analysis of randomized controlled trials.
- Setting and Participants: The analysis included eight eligible trials comprising 600,000 women between the ages of 39 and 74 years.
Bibliographic Data
- Title: Screening for breast cancer with mammography
- Authors: Gøtzsche PC, Jørgensen KJ
- Journal: Cochrane Database of Systematic Reviews
- Year: 2013
- DOI: 10.1002/14651858.CD001877.pub5
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.