
The Wonk Debate – Audio Critique & Clinical Commentary:
🙆♀️🩻Synthesized Clinical Bottom Line
Updated 02-22-2026
The collective evidence—comprising meta-analyses of cohort studies and long-term randomized controlled trials (RCTs)—indicates that the profound survival benefits often attributed to mammography screening in observational data are largely artifacts of Healthy User Bias. While screening successfully identifies more early-stage disease, the evidence suggests that modern systemic therapy and inherent population health drive survival, rather than the technology of earlier detection. The central, unifying theme is that a mammogram is a proxy for the “compliant patient”: women who attend screening possess the socioeconomic and behavioral profiles that reduce their risk of dying from all causes, not just breast cancer.
Key findings supporting this conclusion are:
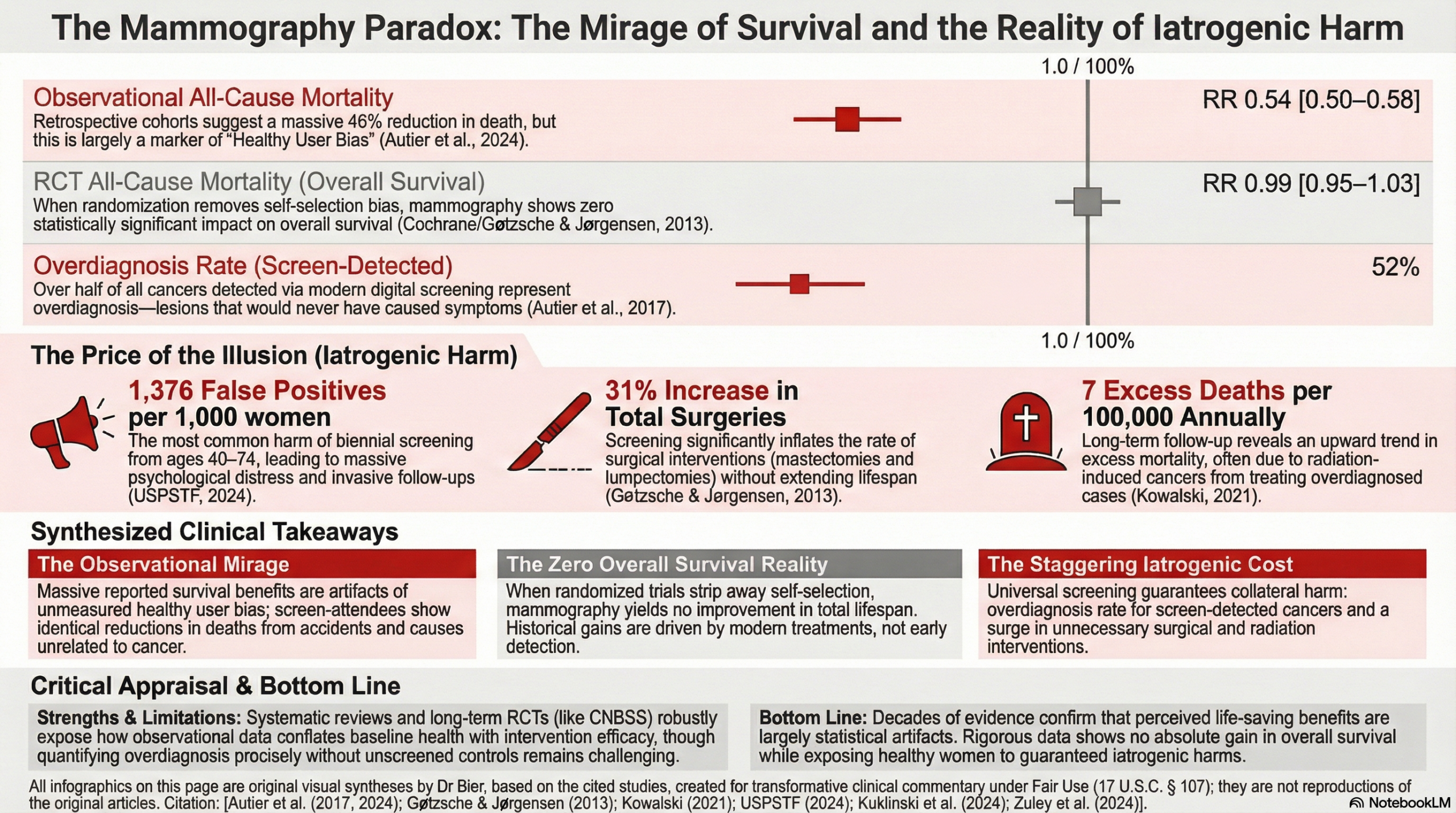
- The Biological Impossibility: Meta-analyses of cohort studies show a 45% reduction in breast cancer mortality alongside a nearly identical 46% reduction in all-cause mortality. Because a breast X-ray cannot biologically prevent death from accidents, heart disease, or other cancers, the reported “benefit” is fundamentally a marker of a healthier baseline population.
- The Zuley Paradox: Higher-frequency (annual) screening appears superior to biennial screening for overall survival (HR = 1.42). This benefit scales with patient compliance rather than clinical intervention; there is no mechanistic basis for annual imaging to reduce non-breast cancer mortality more effectively than biennial imaging.
- The RCT/Observational Conflict: Rigorous RCT data, which eliminates self-selection bias, shows no significant impact on all-cause mortality (RR = 0.99), whereas observational programs (like the Swiss “Donna” program) report survival hazards so low (HR = 0.550) they are statistically incompatible with the known mortality burden of breast cancer.
Thematic Evidence Analysis
1. Healthy User Bias: The “Off-Target” Benefit
The most significant evidence for bias comes from Autier et al. (2024), which exposes what we can call the ‘Accident Paradox.’ Their systematic review of 13 cohort studies found that screening attendees had a 45% lower risk of breast cancer death (RR = 0.55) but also a nearly identical 46% lower risk of death from all other causes (RR = 0.54). This finding identifies a Biological Impossibility: a mammogram has no mechanism to prevent a car crash, a stroke, or a house fire. These identical ‘benefits’ prove that observational studies are not measuring the clinical efficacy of a tool, but are instead documenting the ‘Scout Effect’—the inherent resilience and proactivity of the women who choose to attend. If screening truly drove survival, the reduction in breast cancer deaths would far exceed the reduction in all-cause mortality; the fact that they are mirrors of each other suggests we are simply measuring a marker of a healthy population.
2. The Compliance Gradient: Frequency vs. Resolution
The Zuley et al. (2024) study inadvertently provides the “smoking gun” for this phenomenon. By reporting that annual screening is significantly superior to biennial screening for overall survival (HR = 1.42), the data reaches a point of logical collapse. There is no plausible biological mechanism by which an annual X-ray prevents death from cardiovascular disease or respiratory illness more effectively than a biennial one. Instead, ‘annual screening’ serves as a proxy for the ‘compliant patient’—the woman most likely to follow all health recommendations and possess the resources to manage her health holistically.
3. Systemic Overdiagnosis vs. Modern Therapy
While programs like the Swiss “Donna” program (Kuklinski et al., 2024) report spectacular 10-year overall survival rates (91.4% vs. 72.1%), the Cochrane Review (2013) and Kowalski (2021) argue these gains are largely illusory. The massive rise in early-stage diagnoses has not been met with a corresponding drop in late-stage disease or total mortality in population-level RCTs.
This dynamic is perfectly quantified by Autier et al. (2017) in their 23-year analysis of the Dutch screening program. While national breast cancer mortality fell by 38%, a staggering 85% of that improvement was driven by advances in modern treatment, with screening accounting for a negligible 0% to 5%. Applying a biological plausibility filter, if screening were the primary driver of survival, we would see a sharp decline in advanced disease. Instead, the Dutch data demonstrated that the incidence of stage 2–4 cancers remained virtually identical (shifting from 168 to 166 per 100,000), even as digital mammography triggered a sixfold increase in the detection of in situ lesions.
As systemic treatments have improved, the mortality “benefit” of finding a tumor a few months earlier has been entirely neutralized. Consequently, the primary clinical effect of aggressive screening in these healthy populations is not a reduction in death, but a massive iatrogenic tax. The evidence confirms that 52% of all screen-detected cancers in the digital era are overdiagnosed, creating a devastating 14:1 harm-to-benefit ratio where 14 healthy women are subjected to unnecessary surgery and radiation for every one life potentially saved. Kowalski (2021) provides the long-term data from the Canadian National Breast Screening Study (CNBSS), which reveals an upward-sloping trend of 7 excess deaths per 100,000 women annually. These are not breast cancer deaths; over half of these excess fatalities are attributed to radiation-induced lung and esophageal cancers—the direct result of treating indolent, overdiagnosed lesions that never would have harmed the patient if left alone.
Overall Assessment of the Evidence
The collective evidence builds a consistent narrative: in the era of modern, effective systemic therapy, the survival benefits of mammography screening are over-attributed, and the mortality benefit of early detection, if it ever did exist, no longer does. The primary conflict—the massive survival gaps seen in observational data—is effectively resolved by identifying Healthy User Bias. These studies do not prove that screening saves lives; they prove that women who are healthy enough and compliant enough to be screened regularly are less likely to die of everything. Prioritizing hard clinical endpoints requires us to acknowledge that when a screening model carries a significant harm-to-benefit ratio without moving the needle on overall survival, it functions primarily as a Cause-of-Death shift in statistics rather than a tool for extending life. We are likely over-treating a healthier-than-average population while attributing their natural longevity to the screening and subsequent treatment.
List of Analyzed Papers
- Autier et al. (2024): Effect of screening mammography on the risk of breast cancer deaths and of all-cause deaths. Journal of Clinical Epidemiology.
- Zuley et al. (2024): Breast Cancer Screening Interval: Effect on Rate of Late-Stage Disease at Diagnosis and Overall Survival. Journal of Clinical Oncology.
- Kuklinski et al. (2024): Breast cancer patients enrolled in the Swiss mammography screening program “donna” demonstrate prolonged survival. Breast Cancer Research.
- USPSTF (2024): Screening for Breast Cancer: US Preventive Services Task Force Recommendation Statement. JAMA.
- Gøtzsche & Jørgensen (2013): Screening for breast cancer with mammography. Cochrane Database of Systematic Reviews.
- Kowalski (2021): Mammograms and Mortality: How Has the Evidence Evolved? Journal of Economic Perspectives.
- Autier et al. (2017) Effectiveness of and overdiagnosis from mammography screening in the Netherlands: population based study. BMJ
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.