
Comment:
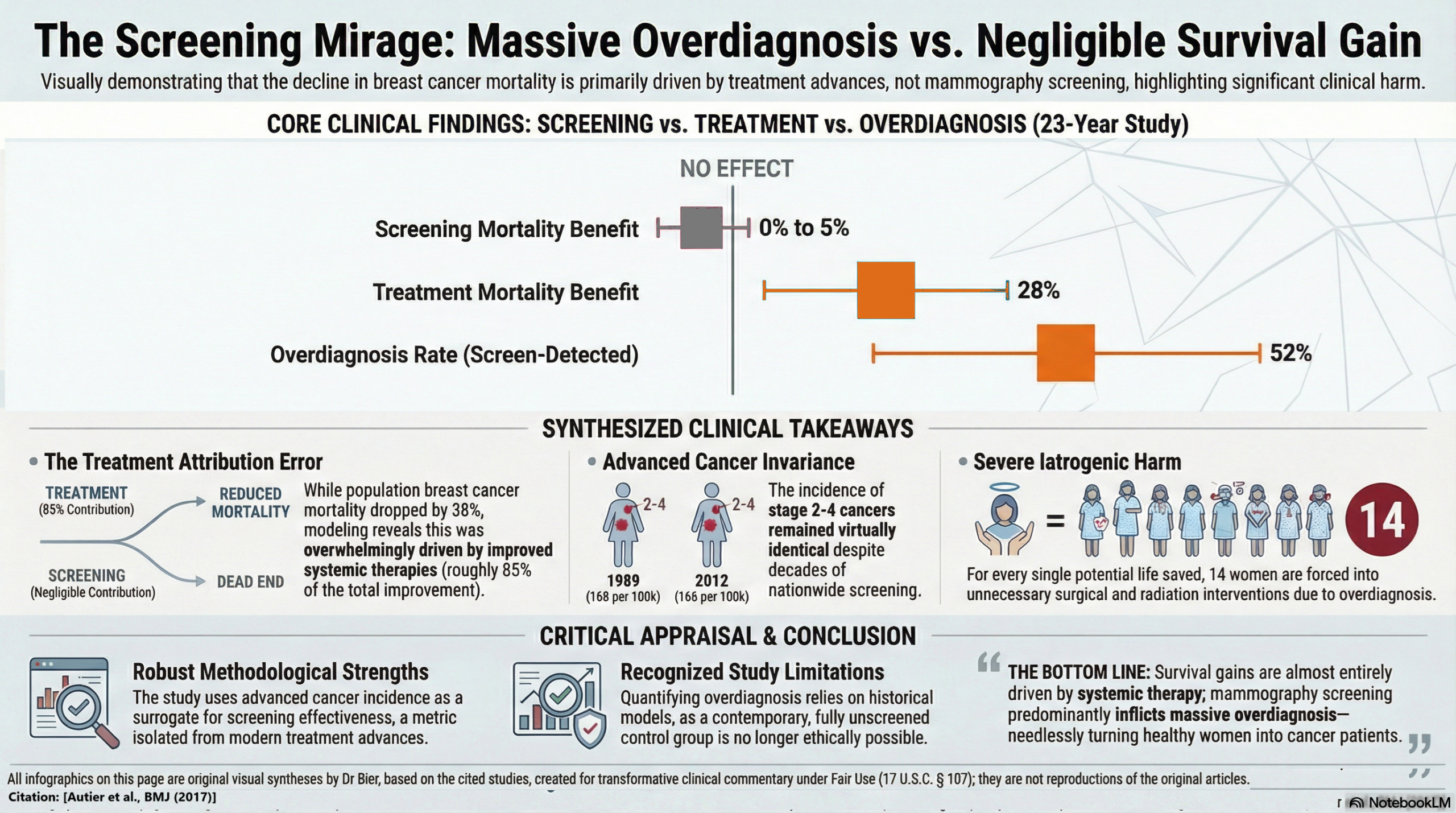
The traditional clinical focus on “detecting cancer early” ignores the underlying reality that “saving a life” in observational data is often a statistical artifact as screening has almost no impact on absolute survival. This 2017 population study from the Netherlands deconstructs a 23-year dataset to reveal a staggering truth: while breast cancer mortality (not overall mortality) fell by 38%, a massive 85% of that improvement was driven by advances in treatment, while screening accounted for a negligible 0% to 5%. We should recognize that the “life-saving” narrative is a documentation of a self-selection artifact; the incidence of advanced (stage 2–4) cancers remained virtually identical from 1989 to 2012.
It also highlights a devastating harm-to-benefit ratio: for every one woman who potentially avoids a breast cancer death, 14 others are overdiagnosed and channeled into unnecessary mastectomies and radiation. While other studies have also shown overdiagnosis, this data shows 52% of all screen-detected cancers in the digital mammography era are overdiagnosed. More sensitive imaging does not equate to better outcomes; instead, it triggers a sixfold increase in in situ lesions without a reciprocal drop in the advanced disease that actually kills.
Summary:
Clinical Bottom Line
This large-scale observational study suggests that 23 years of nationwide mammography screening in the Netherlands has had a marginal impact on reducing advanced breast cancer incidence and, by extension, a negligible effect on breast cancer mortality. While breast cancer mortality in the Netherlands fell by approximately 38% between 1989 and 2013, this study attributes the vast majority (roughly 85%) of that improvement to advances in treatment rather than screening. Most notably, the data indicate a substantial “harm” in the form of massive overdiagnosis: approximately 52% of screen-detected cancers in the digital mammography era likely represent overdiagnosis—tumors that would never have caused clinical symptoms during a woman’s lifetime. For every one life saved by screening, approximately 14 women are overdiagnosed and likely subjected to unnecessary treatment.
Results in Context
- Main Results (Advanced Cancer Incidence): The incidence of stage 2–4 (advanced) breast cancers in women aged >50 remained virtually unchanged, shifting from 168 per 100,000 in 1989 to 166 per 100,000 in 2012.
- Mortality Reductions: After adjusting for temporal trends, screening was associated with a 0% to 5% reduction in breast cancer mortality. In contrast, improved patient management and treatments were associated with a 28% reduction.
- Overdiagnosis Estimates: In the 2010–2012 period, approximately 32% of all breast cancers diagnosed in the invited age group (50–74) were classified as overdiagnosis.
- Definitions: * Overdiagnosis: The detection of cancers through screening that would not have become clinically apparent or caused death during the patient’s lifetime in the absence of screening.
- Advanced Cancers (Stage 2–4): Tumors >20 mm in diameter or those with lymph node/distant metastases; a decrease in these is the primary indicator of screening effectiveness.
- Participants: The study analyzed Dutch women of all ages from 1989 to 2012, encompassing the inception and expansion of the national screening program.
Assertive Critical Appraisal
- Limitations & Bias (STROBE Framework): * Confounding by Treatment: The study effectively uses the incidence of advanced cancers as a surrogate for screening effectiveness because this metric is independent of treatment improvements. The stable incidence of stage 2–4 disease despite high screening participation (80%) strongly undermines the claim that screening is the primary driver of mortality declines.
- Lead Time Bias: The authors appropriately subtracted estimated “lead time” cancers (those destined to become advanced but caught early) from their overdiagnosis calculations to avoid overestimating the harm.
- Reporting Quality Assessment (STROBE): The authors provide a detailed description of their efforts to address confounding, particularly by using age groups not invited to screening (women <50 and >75) as “control” proxies to establish expected incidence trends in the absence of an intervention.
- Reporting Quality Assessment (RECORD): The data sources (WHO mortality database and the Netherlands Cancer Registry) are well-validated and described. However, the lack of a contemporary “unscreened” population limits the study to historical and age-group comparisons, which the authors acknowledge.
- Applicability: These findings are highly relevant to modern clinical practice, especially as the transition to digital mammography was shown to further increase the detection of low-risk in situ lesions (a sixfold increase since 1989) without a reciprocal drop in advanced cancers.
Research Objective
To analyze stage-specific incidence of breast cancer and breast cancer mortality in the Netherlands to quantify the effectiveness of the national mammography program and the extent of overdiagnosis.
Study Design
A population-based observational study utilizing joinpoint regression and age-period-cohort modeling to analyze longitudinal data from national cancer and mortality registries.
Setting and Participants
The nationwide Dutch mammography screening program. Participants included all Dutch women (1989–2012), focusing on those aged 50–75 invited to biennial screening.
Bibliographic Data
- Title: Effectiveness of and overdiagnosis from mammography screening in the Netherlands: population based study
- Authors: Philippe Autier, Magali Boniol, Alice Koechlin, Cécile Pizot, Mathieu Boniol
- Journal: BMJ
- Year: 2017
- DOI: 10.1136/bmj.j5224
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.