
Comment:
This paper serves as a major wake-up call regarding the risks of thyroid replacement in SR+ breast cancer, which compromises about 80% of cases. The mechanistic finding—that thyroid hormone can reverse Tamoxifen’s action from antagonist to agonist—is a critical piece of the puzzle explaining treatment failure. Furthermore, the observation that Aromatase Inhibitors also showed significantly higher failure rates (14% vs. 2%) suggests that the risk is pervasive across endocrine therapies. It compels us to view thyroid hormone not as a neutral background factor, but as a potent variable that will significantly alter long-term patient outcomes.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
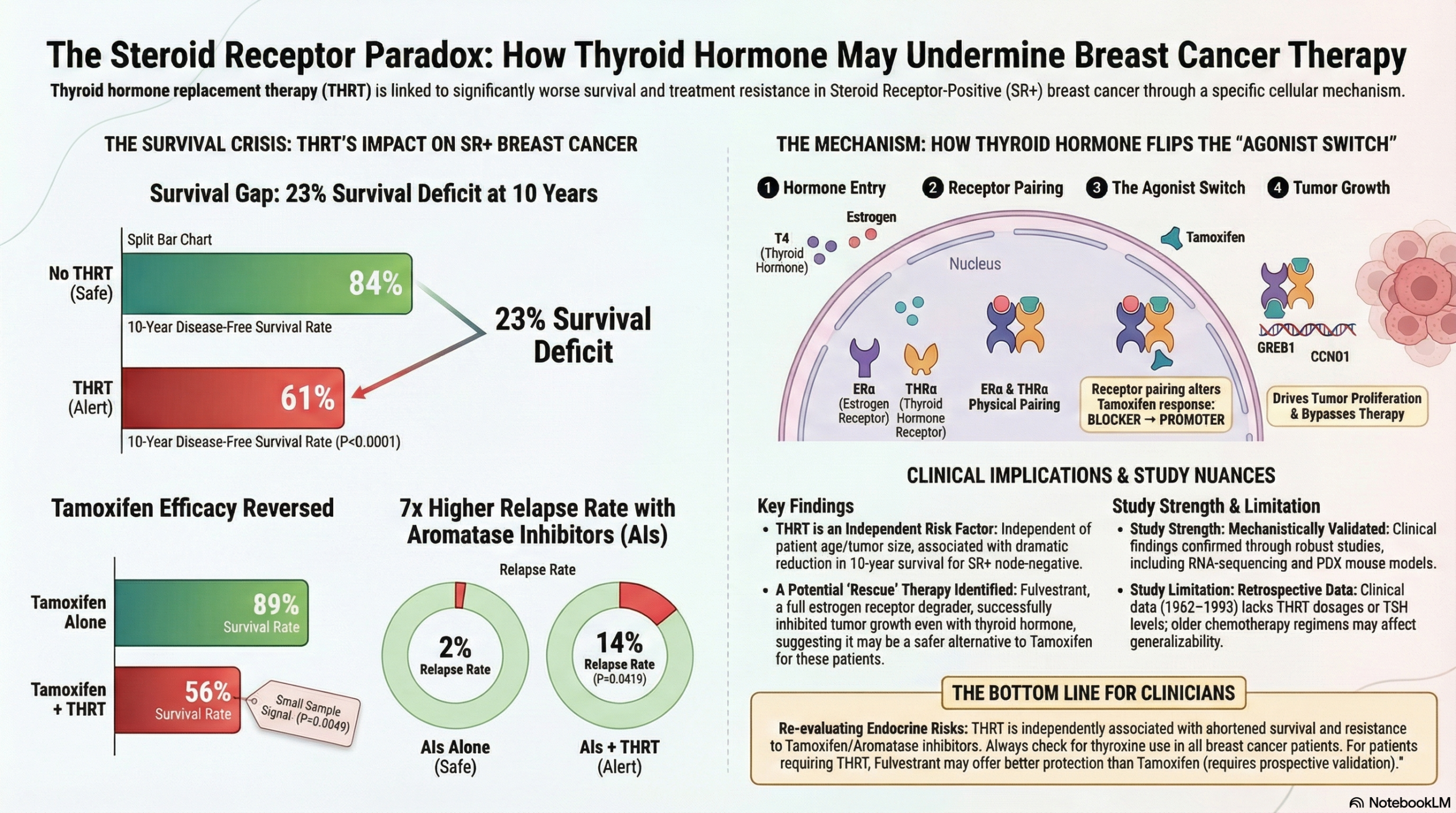
This study provides compelling evidence that Thyroid Hormone Replacement Therapy (THRT) is independently associated with significantly shortened disease-free and disease-specific survival in women with Steroid Receptor-positive (SR+) lymph node-negative breast cancer.
Crucially, the study suggests a specific biological interaction: Thyroid Hormone (TH) appears to induce “cross-talk” between thyroid and estrogen receptors, potentially converting Tamoxifen from an estrogen antagonist (blocker) into an agonist (promoter) in these specific tumors. Clinicians should be aware that SR+ patients receiving both THRT and Tamoxifen experienced the worst outcomes of all treatment groups. While observational, the strong biological plausibility provided by the accompanying animal models suggests that aggressive thyroid hormone management and the choice of endocrine therapy (e.g., considering fulvestrant or aromatase inhibitors over tamoxifen) may warrant closer scrutiny in this population.
Results in Context
- Clinical Outcomes (Observational Cohorts)
- Primary Finding (Cohort 1 – MGH): In a long-term study of 820 patients, THRT significantly reduced Disease-Free Survival (DFS) and Disease-Specific Survival (DSS) only in patients with SR+ tumors.
- 10-Year DFS: 61% for THRT group vs. 84% for the non-THRT group (P<0.0001).
- 10-Year DSS: 76% for THRT group vs. 92% for the non-THRT group (P<0.0001).
- Negative Control: There was no significant difference in survival based on THRT use in patients with SR- (negative) breast cancer, supporting a hormonally driven mechanism.
- The “Tamoxifen Paradox”: Patients with SR+ cancer treated with Tamoxifen + THRT had the shortest survival of all groups (10-year DFS of 56% vs. 89% for Tamoxifen alone).
- Aromatase Inhibitors (Cohort 2 – UCH): In a separate cohort of 160 patients, those treated with Aromatase Inhibitors (AI) + THRT also had significantly shorter DFS compared to AI alone (P=0.0419), with a 14% relapse rate vs. 2% for AI alone.
- Translational & Mechanistic Findings
- Receptor Cross-Talk: In ER^{+} breast cancer cells (MCF7, T47D), treatment with TH and Estrogen (E2) caused nuclear colocalization of the Thyroid Hormone Receptor (THR\alpha) and Estrogen Receptor (ER\alpha). This interaction upregulated proliferative genes (e.g., GREB1, CCND1, MYC). * Tamoxifen Resistance: In mouse models (PDX), Tamoxifen successfully inhibited tumor growth in mice treated with Estrogen alone. However, in mice treated with Estrogen + Thyroid Hormone, Tamoxifen failed to inhibit growth, acting instead as a proliferative agonist.
- Rescue with Fulvestrant: Unlike Tamoxifen, Fulvestrant (a full ER degrader) successfully attenuated tumor growth even in the presence of Thyroid Hormone.
- Gene Signatures: Tumors treated with E2 + TH showed significant upregulation of high-risk genes found in commercial prognostic assays (Oncotype DX, MammaPrint, EndoPredict), suggesting TH drives the tumor biology toward a “high risk” profile.
Assertive Critical Appraisal
Limitations & Bias (STROBE & Translational)
- Retrospective Design: The clinical data is retrospective. Cohort 1 spans 1962–1993, a period where chemotherapy regimens and systemic therapies differed significantly from modern standards (e.g., lower Doxorubicin doses).
- Sample Size in Subgroups: While the overall cohort was large (n=820), the specific subgroup of “Tamoxifen + THRT” was small (n=9 in Cohort 1). While the statistical signal was strong (P=0.0049), the small number of events warrants caution in interpreting the magnitude of the risk.
- Confounding Variables: The authors performed multivariate analysis controlling for age, tumor size, and grade. THRT remained an independent predictor of poor DFS (P=0.03) and 10-year survival statistics. However, detailed data on thyroid hormone dosages or TSH levels were not granularly analyzed in the clinical cohorts, which is a common limitation in retrospective chart reviews.
Reporting Quality Assessment
- STROBE/REMARK: The authors provide a clear flow diagram (REMARK) for patient inclusion/exclusion.
- Supplementary Transparency: The supplementary data transparently displays the specific breakdown of surgical approaches (mastectomy vs. lumpectomy) and confirms that surgical type did not alter the THRT-associated risk.
- Bioinformatics Rigor: The study validates its gene expression findings across multiple public datasets (TCGA, Curtis, Finak), strengthening the claim that THR\alpha expression correlates with poor outcomes in SR+ cancer.
Applicability
This study has high clinical relevance given that hypothyroidism is a frequent comorbidity in breast cancer, and approximately 1/3 of patients may utilize THRT. The findings suggest that for SR+ patients, TSH suppression (keeping thyroid hormone levels high) might be counterproductive. It specifically raises the hypothesis that Fulvestrant or Aromatase Inhibitors might be safer than Tamoxifen for women requiring THRT, though prospective validation is needed.
Research Objective
To determine whether Thyroid Hormone Replacement Therapy (THRT) influences survival outcomes in lymph node-negative breast cancer and to elucidate the molecular mechanisms underlying any observed interactions between thyroid hormone and estrogen signaling.
Study Design
- Part 1: Retrospective Observational Cohort Study (Two independent cohorts).
- Part 2: In vivo (Patient-Derived Xenograft mice) and in vitro (cell line) mechanistic studies using RNA-seq and gene expression profiling.
Setting and Participants
- Cohort 1: 820 patients with lymph node-negative (LN-) breast cancer treated at Massachusetts General Hospital (MGH) between 1962–1993.
- Cohort 2: 160 postmenopausal patients with Stage I, LN- breast cancer treated at University of Colorado Hospital (UCH) between 2006–2009.
- Models: MCF7, T47D, and PT12 breast cancer cell lines; NSG mice for xenograft studies.
Bibliographic Data
- Authors: Wahdan-Alaswad RS, Edgerton SM, Salem H, et al.
- Journal: Clinical Cancer Research
- Year: 2021
- DOI: 10.1158/1078-0432.CCR-20-2647
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.