
Comment:
Yet another study challenging the safety profile of synthetic T4. The data here is sobering: thyroid cancer survivors on high-dose levothyroxine faced significantly higher risks of developing a second unrelated (not recurrence) cancer, particularly in the GI tract. With hazard ratios for pancreatic, liver cancers reaching nearly 2.5 and 2.0 respectively, this is a safety signal that warrants immediate attention. There is also a 1.6 hazard ratio for colorectal cancer, which is smaller, but for a very frequent cancer, quite concerning. It again supports the perspective that synthetic monotherapy is not a neutral replacement, but a potent intervention with off-target effects that can significantly alter long-term patient outcomes.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
This large retrospective cohort study identifies a dose-dependent association between high-dose levothyroxine use and an increased risk of subsequent primary cancers (SPCs) in thyroid cancer survivors, specifically gastrointestinal, hepato-biliary, and pancreatic malignancies. While this observational design cannot prove causation, and the study relies on drug dosage rather than serum TSH levels, the findings suggest that aggressive TSH suppression strategies should be carefully tailored, weighing potential oncologic benefits against long-term toxicity risks.
Results in Context
Main Results
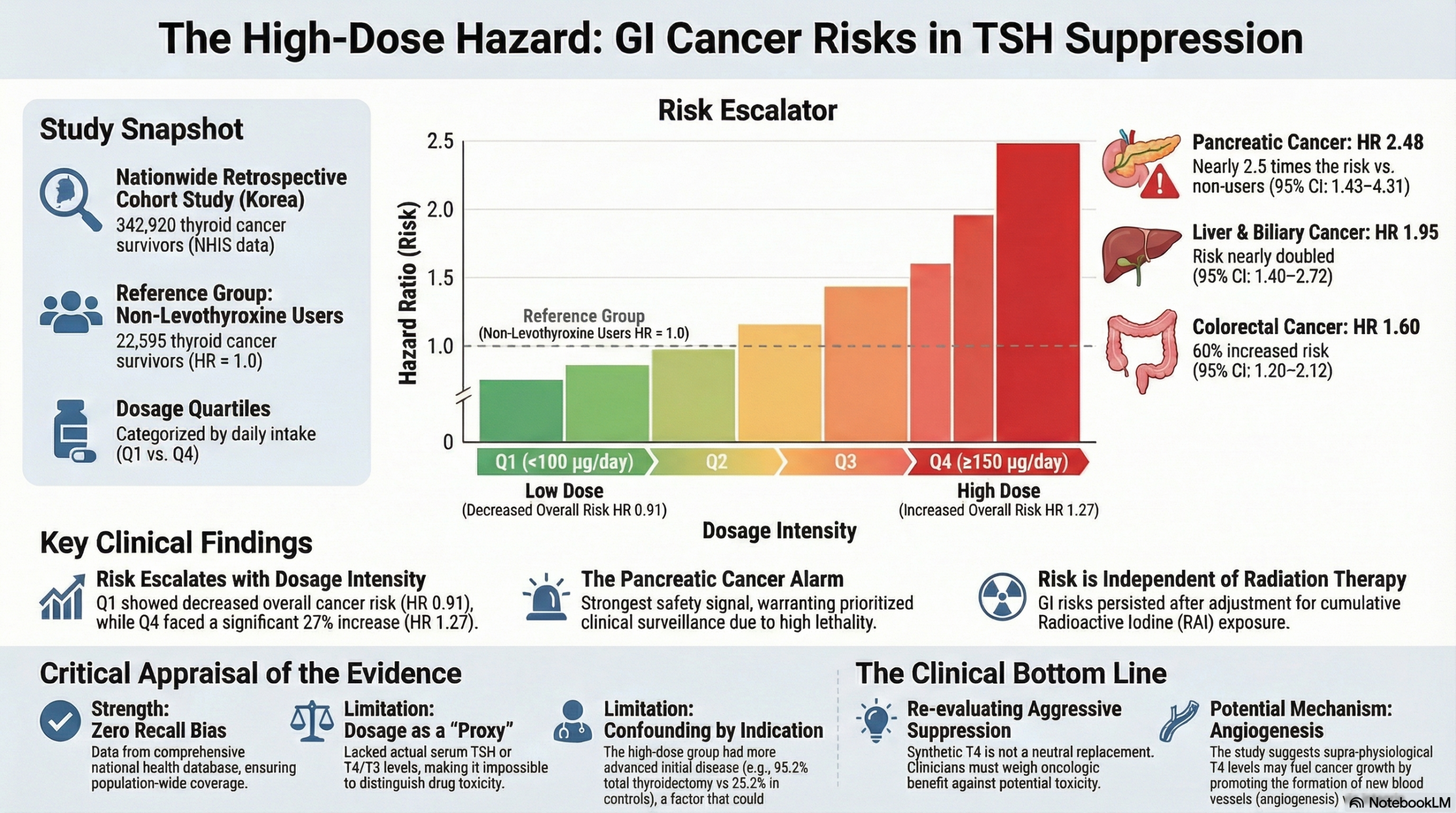
The study compared thyroid cancer survivors taking levothyroxine to a non-levothyroxine control group. The analysis revealed a statistically significant, dose-dependent increase in cancer risk:
- Overall SPC Risk: Patients in the highest dosage quartile (Q4) had a 27% higher risk of developing a subsequent primary cancer compared to the non-levothyroxine group (HR = 1.27; 95% CI, 1.17–1.37).
- Specific Organ Risks (Q4 Group): The risk elevation was most pronounced for digestive system cancers:
- Pancreatic Cancer: Risk increased by nearly 2.5 times (HR = 2.48; 95% CI, 1.43–4.31).
- Liver and Biliary Tract: Risk increased by nearly 2-fold (HR = 1.95; 95% CI, 1.40–2.72).
- Colorectal Cancer: Risk increased by 60% (HR = 1.60; 95% CI, 1.20–2.12).
- Stomach Cancer: Risk increased by 31% (HR = 1.31; 95% CI, 1.01–1.71).
Definitions
- Hazard Ratio (HR): An HR of 1.27 indicates that the event rate (cancer diagnosis) in the high-dose group was 1.27 times the rate in the control group.
- Quartiles (Q1-Q4): Dosage groups were divided by daily intake: Q1 (<100 µg/day), Q2 (100–123 µg/day), Q3 (124–149 µg/day), and Q4 (≥150 µg/day).
Participants
The study analyzed 342,920 patients who underwent thyroidectomy. This included a non-levothyroxine group (n=22,595) and a levothyroxine group (n=320,325).
Assertive Critical Appraisal
Limitations & Bias (STROBE Framework)
- Proxy Measurement Validity (Major Limitation): The study uses levothyroxine dosage as a proxy for TSH suppression but did not report actual serum TSH or thyroid hormone levels. This is a critical flaw; without biochemical data, it is impossible to determine if the increased cancer risk is due to low TSH (suppression) or high circulating thyroxine (drug effect).
- Confounding by Indication: Patients prescribed higher doses of levothyroxine (Q4) had significantly higher rates of total thyroidectomy (95.2% vs. 25.2%) and radioactive iodine (RAI) therapy (61.4% vs. 0%) compared to the non-levothyroxine group. This suggests the high-dose group had more advanced disease. While the authors adjusted for cumulative RAI doses, residual confounding by disease severity or surveillance bias (more frequent imaging in high-risk patients) remains a threat to validity.
- Missing Clinical Data: The database lacked information on tumor stage, which could lead to residual confounding.
Reporting Quality Assessment (STROBE)
- Handling of Confounders: The authors adequately employed Cox proportional hazard models to adjust for age, sex, comorbidities (Charlson Comorbidity Index), obesity, smoking, and alcohol consumption.
- Sensitivity Analyses: The authors strengthened their findings by performing subgroup analyses on patients with good medication adherence (MPR \ge 80\%) and by stratifying for RAI therapy, which showed consistent results. This robustness check helps mitigate concerns regarding medication compliance.
Applicability
This study was conducted using the Korean National Health Insurance database. While the physiological mechanisms of thyroid hormone are universal, genetic or environmental factors (e.g., diet, gastric cancer prevalence) specific to the Korean population may limit generalizability to Western populations.
Study Details
Research Objective
To investigate the association between levothyroxine dosage and the risk for subsequent primary cancers (SPCs) in thyroid cancer patients, specifically adjusting for the effect of radioactive iodine (RAI) therapy.
Study Design
- Design: Nationwide population-based retrospective cohort study.
- Data Source: Korean National Health Insurance Service (NHIS) database.
- Follow-up: Median follow-up of 7.3 years.
Setting and Participants
- Inclusion: Patients newly diagnosed with thyroid cancer (ICD-10 C73) who underwent thyroidectomy between January 2004 and December 2018.
- Exclusion: Patients with antecedent malignancies within 2 years of diagnosis or a history of levothyroxine use prior to thyroid cancer diagnosis.
Bibliographic Data
- Authors: Min-Su Kim, Jang Won Lee, Min Kyung Hyun, Young Shin Song
- Journal: Endocrinology and Metabolism (EnM)
- Year: 2024
- DOI: 10.3803/EnM.2023.1815
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.