
Comment:
This study provides a fascinating glimpse into the potential of ‘precision nutrition’—where efficacy may depend entirely on the tumor’s specific genomic profile which we now have information on. The finding that Vitamin C intake improves survival specifically and only in KRAS and BRAF mutated tumors aligns perfectly with the known biology: these mutations upregulate GLUT1, effectively tricking the cancer cell into importing lethal amounts of oxidized Vitamin C.
While we always must remain cautious of the ‘healthy user effect’ inherent in observational data, the strong biological plausibility here increases the likelihood the effect is real. Although this study was on oral vitamin C intake, it also points to a potential differentiation for intravenous ascorbic acid as well.
However, the study failed to show an improvement in overall survival even in the mutated group, which blunts our enthusiasm somewhat for the findings.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
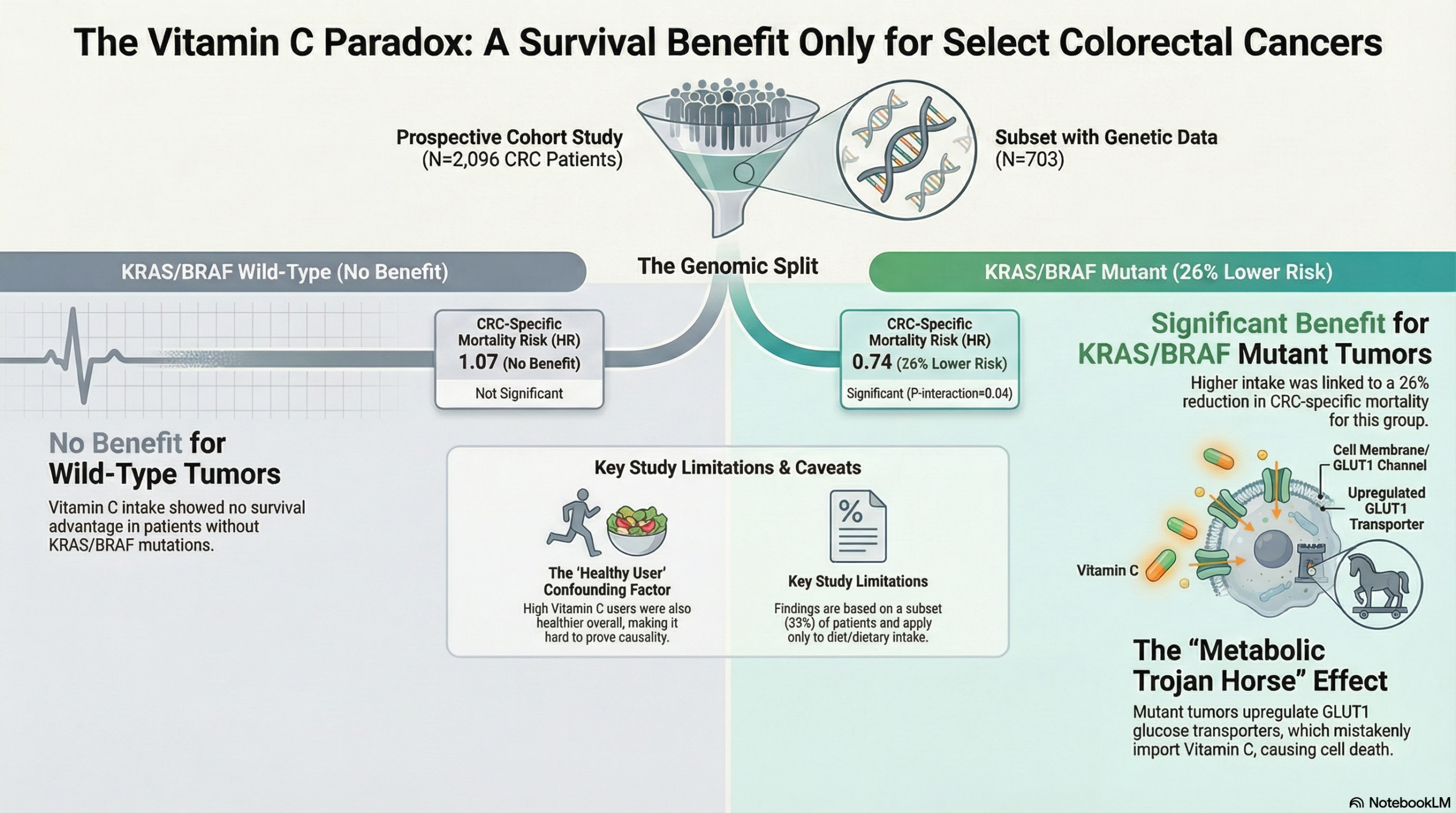
This prospective cohort study identifies a biologically plausible interaction between post-diagnostic Vitamin C intake and colorectal cancer (CRC) survival. The authors found that higher Vitamin C intake is associated with reduced CRC-specific mortality specifically in patients with KRAS or BRAF mutations, but not in those with wild-type tumors.
While these findings are supported by mechanistic data showing that KRAS/BRAF mutations upregulate the GLUT1 transporter (facilitating Vitamin C uptake), this is an observational study. Therefore, causality cannot be established due to the potential for residual confounding (e.g., patients taking high Vitamin C generally had healthier lifestyles). Clinicians should view this as hypothesis-generating evidence that supports the potential role of Vitamin C as an adjuvant strategy in mutant CRC, rather than a directive for immediate practice change.
Results in Context
Main Results
CRC Cancer Specific Mortality
- Overall Cohort: In the total population of 2,096 CRC patients, post-diagnostic total Vitamin C intake was not associated with CRC-specific mortality (P-trend=0.88) or all-cause mortality (P-trend=0.85).
- Mutation-Specific Interaction: There was a statistically significant interaction between Vitamin C intake and mutation status (P-interaction=0.04).
- Wild-Type: No association was found. The multivariable Hazard Ratio (HR) per 400 mg/day increase was 1.07 (95% CI: 0.87-1.32).
- KRAS/BRAF Mutant: A significant inverse association was observed. The HR per 400 mg/day increase was 0.74 (95% CI: 0.55-1.00; P-trend < 0.05).
- Mechanistic Validation (TCGA Analysis): Analysis of The Cancer Genome Atlas (TCGA) database confirmed that KRAS or BRAF mutated tumors have significantly higher mRNA expression of SLC2A1 (the gene encoding the GLUT1 transporter) compared to wild-type tumors (P=0.02).
Overall Mortality
-
Overall Cohort (No association):
In the total population of 2,096 patients, post-diagnostic Vitamin C intake was not associated with all-cause mortality. The hazard ratio (HR) per 400 mg/day increase was 0.99 (95% CI: 0.95–1.05; P-trend=0.85), indicating no survival benefit when looking at deaths from any cause3.
-
KRAS/BRAF Subgroups (No association):
Unlike the specific benefit seen for colorectal cancer death, there was no significant interaction between Vitamin C intake and mutation status for all-cause mortality ($P_{interaction}=0.99$)4.
-
Wild Type: HR 0.96 (0.86–1.06).
-
Mutant Type: HR 0.96 (0.87–1.07).
-
Definitions
- Hazard Ratio (HR): A measure of how often a particular event (in this case, death) happens in one group compared to another over time. An HR of 0.74 implies a 26% reduction in the rate of specific mortality in the group with higher intake compared to lower intake.
- Interaction (P-interaction): A statistical test to determine if the effect of the exposure (Vitamin C) differs significantly between subgroups (Mutant vs. Wild-type).
Participants
- The study included 2,096 patients with incident stage I-III CRC from the Nurses’ Health Study and Health Professionals Follow-up Study.
- Of these, 703 cases had available KRAS and BRAF mutation data.
Assertive Critical Appraisal
Limitations & Bias (STROBE Framework)
- Selection Bias (Missing Tumor Data): Only 703 of the 2,096 identified cases (approx. 33%) had mutation data available. While the authors noted that lifestyle characteristics were similar between those with and without tumor data, analyzing a subset reduces power and introduces potential selection bias if tissue availability correlates with other unmeasured factors.
- Confounding: Participants with higher Vitamin C intake had distinctly healthier profiles: they were more physically active, had higher intakes of fiber and vitamin D, and used aspirin more frequently. While the authors utilized a robust multivariable model adjusting for these factors, residual confounding by a “healthy user effect” remains the most significant threat to validity in nutritional epidemiology.
- Measurement Error: Vitamin C intake was assessed via Food Frequency Questionnaires (FFQs). While validated, self-reported dietary data is subject to recall bias and measurement error, though the authors correctly note that prospective collection likely biases results toward the null (underestimation of effect) rather than creating a false positive.
Reporting Quality Assessment (STROBE)
- Addressing Bias: The authors employed Inverse Probability Weighting (IPW) to account for the unavailability of tumor tissue data. This is a rigorous statistical technique that strengthens the reliability of the subgroup analysis by re-weighting the available data to represent the full cohort.
- Dose-Response: The authors appropriately used spline analysis to check for non-linear relationships. They found a linear relationship up to 1000 mg/day, acknowledging that they lacked data on high-dose IV Vitamin C used in some clinical trials.
Applicability
- The cohorts are predominantly white health professionals. While the biological mechanism involving KRAS and GLUT1 is likely universal, socio-economic and dietary baselines may differ in the general population.
- The results apply to dietary and supplemental intake (up to 1000 mg/day), not high-dose intravenous therapy often discussed in integrative oncology.
Research Objective
The study aimed to examine the prospective association of post-diagnostic Vitamin C intake with CRC-specific and all-cause mortality, specifically stratified by tumor KRAS or BRAF mutation status.
Study Design
- Design: Prospective Cohort Study (pooled analysis of two cohorts).
- Key Statistical Methods: Inverse probability weighted multivariable Cox proportional hazards regression; Restricted cubic splines for dose-response.
Setting and Participants
- Setting: Two large US cohorts: The Nurses’ Health Study (NHS, women) and the Health Professionals Follow-up Study (HPFS, men).
- Eligibility: Participants diagnosed with incident stage I-III colorectal cancer during follow-up.
- Follow-up: Average of 12.0 years.
Bibliographic Data
- Title: Vitamin C intake and colorectal cancer survival according to KRAS and BRAF mutation: a prospective study in two US cohorts
- Authors: Shi S, Wang K, Ugai T, Giannakis M, et al.
- Journal: British Journal of Cancer
- Year: 2023
- DOI: 10.1038/s41416-023-02452-2
Original Article:
Full text: Pubmed Central
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.