
Comment:
This synthesis serves as a robust rebuttal to the long-standing “precautions” that have dominated lymphedema education. The findings demonstrate that most traditional prohibitions—specifically air travel and blood pressure measurements—are effectively myths that lack Level 1 or 2 evidence. The core tension is between a historical focus with these external triggers and the clinical reality that only cellulitis stands as a validated, independent risk factor. It reinforces that we must stop viewing routine medical interventions as primary drivers of risk when the human data shows no significant association with increased arm volume.
The tangible significance for the patient is the immediate removal of unnecessary psychological and medical burden. By acknowledging that the “at-risk” arm is not nearly as fragile as we feared, we can integrate standard care practices without fear of triggering breast cancer-related lymphedema (BCRL).
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line:
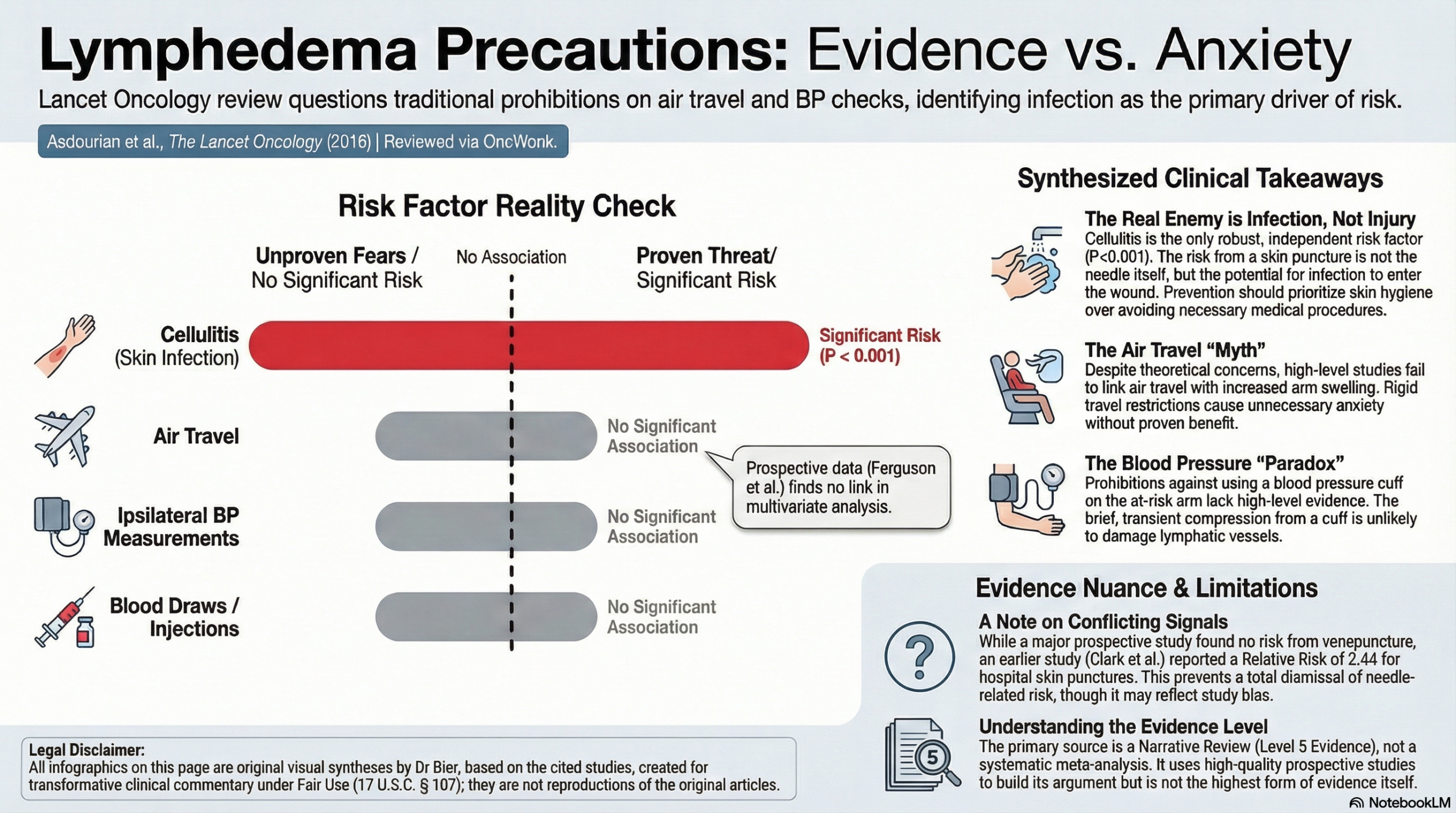
This review argues that the precautionary guidelines historically given to breast cancer survivors—specifically regarding air travel, blood pressure measurements, and skin punctures on the ipsilateral arm—are largely unsubstantiated by high-level scientific evidence. The authors contend that while skin infection (cellulitis) is a well-established risk factor, other external “lifestyle” triggers lack consistent causal data. Consequently, the authors suggest that rigid adherence to these restrictions may cause unnecessary patient anxiety and medical inconvenience, advocating instead for a risk-stratified approach to precautions rather than a “one-size-fits-all” mandate.
Key Themes & Evidence Summary
- Lack of Evidence for Air Travel and Compression
- The Findings: The review identifies a lack of consensus regarding air travel as a trigger for lymphoedema. While theoretical risks exist (hypobaric-hypoxic environments), prospective studies largely fail to show a significant association between flight and arm volume increase.
- Compression Garments: The utility of prophylactic compression sleeves during flight is debated. One study suggested that using precautions (like sleeves) was actually associated with higher lymphoedema risk, potentially because those patients were more hyper-vigilant or had sub-clinical symptoms. The review concludes that for at-risk women, there is no definitive evidence that compression confers a benefit during travel.
- Ipsilateral Blood Pressure (BP) and Limb Constriction
- The Findings: Despite the common prohibition against checking BP on the at-risk arm, the review found no Level 1 or 2 evidence linking isolated BP measurements to lymphoedema onset.
- Data conflicts: While one retrospective study (Level 4) showed a prevalence increase with ipsilateral BP checks, prospective studies did not find this association significant in multivariate analyses. The authors argue that brief constriction from a BP cuff is unlikely to damage lymphatic vessels compared to sustained pressure.
- Skin Puncture (Venepuncture/Injections)
- The Findings: Evidence here is conflicting. One prospective study (Level 2) did find a relative risk of 2.44 for lymphoedema following hospital skin puncture. However, the authors note this study may be subject to recall bias.
- Infection vs. Puncture: Other prospective analyses found no significant association between blood draws/infusions and arm swelling. The review suggests the risk likely stems from subsequent infection (cellulitis) entering through the skin break, rather than the mechanical trauma of the needle itself.
- Extreme Temperatures
- The Findings: Evidence linking temperature extremes to lymphoedema is scarce. One study linked sauna use to swelling, but this was confounded by the presence of skin cuts on the arm.
- Heat Therapy: Interestingly, the review notes that microwave heat therapy has been used safely in some trials to treat lymphoedema, contradicting the blanket advice to avoid heat.
- Cellulitis: The Validated Risk
- The Findings: In contrast to the factors above, skin infection (cellulitis) is consistently identified as a significant, independent risk factor for the development and worsening of lymphoedema.
- Mechanism: A vicious cycle exists where lymphoedema predisposes to infection, and infection further damages lymphatic vessels, exacerbating swelling.
Assertive Critical Appraisal
- Evidence Level: Narrative Review (Level 5 Evidence). While the authors utilized a grading system (Levels 1–5) to evaluate included studies, the document itself is a narrative synthesis rather than a systematic meta-analysis with pooled statistical estimates.
- Quality Assessment (SANRA Scale):
- Justification & Aims: The review is well-justified. It addresses a significant clinical gap between rigid guidelines and the “paucity of high-level evidence” supporting them.
- Literature Search: The search strategy is clearly described (PubMed/Google Scholar, Feb–March 2016), enhancing reproducibility.
- Scientific Reasoning: The argument is logical and nuanced. The authors successfully differentiate between biological plausibility (theory) and clinical reality (data). They rightfully critique the reliance on retrospective data, which is prone to recall bias (e.g., patients with swelling are more likely to “remember” a needle stick).
- Proposed Risk Stratification: The authors move beyond simple critique to propose a practical framework. They suggest stratifying precautions based on surgical history:
- High Risk: Axillary Lymph Node Dissection (ALND) + Radiation or BMI $\ge 30~kg/m^{2}$.
- Low Risk: Sentinel Lymph Node Biopsy (SLNB) only, where lymphoedema incidence is $0-6\%$.
- Critique: This stratification is expert opinion, but it represents a sensible application of the data to reduce patient burden.
Research Objective
To review the literature on lifestyle-associated risk factors (air travel, BP measurements, skin puncture, extreme temperatures, cellulitis) and determine if they validly increase the risk of breast cancer-related lymphoedema.
Bibliographic Data
- Title: Precautions for breast cancer-related lymphoedema: risk from air travel, ipsilateral arm blood pressure measurements, skin puncture, extreme temperatures, and cellulitis
- Authors: Asdourian MS, Skolny MN, Brunelle C, Seward CE, Salama L, Taghian AG
- Journal: The Lancet Oncology
- Year: 2016
- DOI: 10.1016/S1470-2045(16)30204-2
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.