
Comment:
This is an interesting and potentially alarming one. I’m sure we’ve all noted times where a stable patient started progressing after getting an infection.
This study shows an association of SARS-CoV-2 infection with a nearly two-fold increase in cancer-specific mortality (UK Biobank) and a 44% higher rate of lung metastases in breast cancer patients (Flatiron).
This provides compelling evidence that COVID infection. and potentially all respiratory viral infections are a plausible and clinically relevant trigger for metastatic relapse, demanding further investigation and potentially heightened surveillance for our patients.
Summary
Clinical Bottom Line
This study’s analysis of two large human databases reveals a concerning association between SARS-CoV-2 infection and an increased risk of both cancer-related mortality and the development of lung metastases in cancer survivors. While this observational data cannot prove causation, it aligns with the study’s pre-clinical findings and strongly suggests that respiratory viral infections could be a clinically relevant trigger for metastatic relapse, particularly in patients with breast cancer.
Results in Context
The study analyzed two independent, real-world datasets to assess the impact of COVID-19 on cancer outcomes.
1. UK Biobank (Cancer Mortality)
-
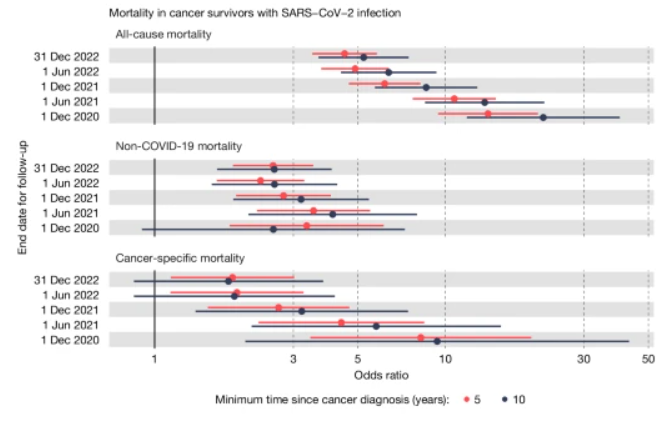
Main Result: Among a matched group of cancer survivors (diagnosed at least five years prior), a positive SARS-CoV-2 test was associated with a nearly twofold increase in the odds of cancer-specific mortality compared to those who tested negative. The association was most pronounced in the first few months following infection and diminished over time.
-
Definitions: The reported odds ratio was 1.85 (95% Confidence Interval: 1.14 to 3.02). An odds ratio of 1.85 means the odds of dying from cancer were 85% higher in the group that tested positive for SARS-CoV-2 compared to the group that tested negative.
2. Flatiron Health Database (Lung Metastasis in Breast Cancer)
-
Main Result: In a large cohort of female breast cancer patients, a COVID-19 diagnosis was associated with a 44% increased rate of subsequent progression to lung metastases.
-
Definitions: The reported hazard ratio was 1.44 (95% Confidence Interval: 1.01 to 2.05). A hazard ratio of 1.44 signifies that at any point during the follow-up period, patients with a COVID-19 diagnosis had a 44% higher rate of developing lung metastases compared to those without a diagnosis.
-
Participants: The UK Biobank analysis included a final matched cohort of 487 COVID-positive and 4,350 COVID-negative cancer survivors. The Flatiron Health analysis included 36,845 female breast cancer patients, of whom 532 had a COVID-19 diagnosis during follow-up.
Assertive Critical Appraisal
-
Limitations & Bias: This is high-quality observational data, but it has inherent limitations. The primary weakness is the potential for information bias. In both databases, the “uninfected” or “negative” comparison groups may have included individuals with undiagnosed or unreported SARS-CoV-2 infections. This type of misclassification would typically bias the results toward the null, meaning the true association between infection and metastatic progression could be even stronger than what was reported.
-
Confounding: The analyses attempted to control for key confounding variables. The UK Biobank study used a rigorous matching strategy for factors like age, sex, and cancer type, while the Flatiron Health analysis adjusted for age, race, comorbidities, and cancer subtype. However, the possibility of unmeasured confounding variables—such as differences in health status or health-seeking behaviors between those who were diagnosed with COVID-19 and those who were not—cannot be entirely excluded.
-
Applicability: The findings are derived from large, real-world patient populations in the UK and the US, enhancing their generalizability to typical clinical practice. The specific focus on lung metastasis in breast cancer survivors in the Flatiron analysis is directly relevant to oncology and primary care settings where these patients are followed.
Research Objective
The objective of the human data analysis was to determine whether SARS-CoV-2 infection is associated with an increased risk of cancer-related mortality and metastatic progression in cancer survivors, using real-world data to test the hypothesis generated from the study’s pre-clinical mouse models.
Study Design
This was a retrospective analysis of two large, independent, real-world databases.
-
UK Biobank: A population-based cohort study. A matched analysis was performed, comparing cancer survivors with a positive SARS-CoV-2 PCR test to those with a negative test.
-
Flatiron Health: A retrospective cohort study using a nationwide electronic health record (EHR) database from US cancer clinics. The analysis treated COVID-19 diagnosis as a time-varying exposure to assess its effect on the risk of developing lung metastases.
Setting and Participants
-
UK Biobank: Participants were adult volunteers in a UK-based longitudinal study. The analysis focused on 4,837 cancer survivors who had their cancer diagnosis at least 5 years before the pandemic and were tested for SARS-CoV-2 before the widespread vaccine rollout.
-
Flatiron Health: The database includes de-identified data from approximately 280 US cancer clinics. The study population consisted of 36,845 female patients with a diagnosis of non-metastatic or metastatic breast cancer.
Bibliographic Data
-
Title: Respiratory viral infections awaken metastatic breast cancer cells in lungs
-
Authors: Shi B. Chia, Bryan J. Johnson, Junxiao Hu, et al.
-
Journal: Nature
-
Year: 2025
Original Article:
Full text: PubMed Central
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.