
Comment:
This study provides the critical ‘why’ behind the findings from this same groups earlier study. In that article, we highlighted that exogenous thyroid hormone is associated with significantly shortened survival in SR+ breast cancer patients. Now, this research explains elucidates the underlying mechanism: thyroid hormone essentially ‘hijacks’ the estrogen receptor, driving proliferation and rendering Tamoxifen effectively useless. It validates that the survival gap seen in the previous study and others isn’t a fluke; it is the result of a physiological mismatch where the thyroid replacement undermines the clinical utility of standard endocrine interventions.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
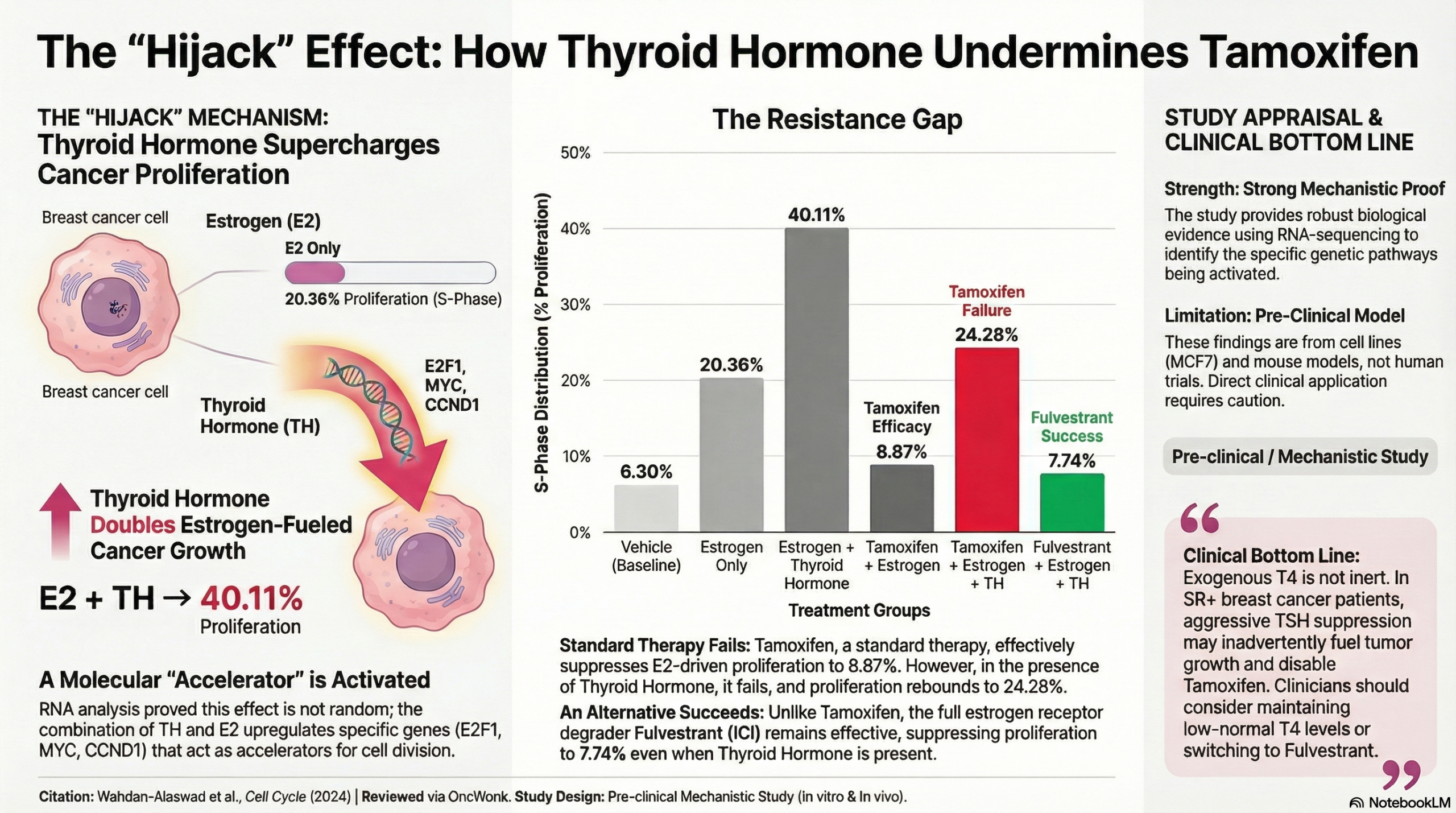
This mechanistic study provides strong biological evidence supporting the link between thyroid hormone (thyroxine/T4 and triiodothyronine/T3) and increased cancer risk in steroid receptor-positive (SR+) breast cancer. The authors demonstrate that thyroid hormone (TH), particularly when combined with estrogen (E2), significantly enhances tumor cell proliferation, reduces apoptosis (programmed cell death), and promotes resistance to tamoxifen therapy1. Clinically, these findings suggest that exogenous thyroxine replacement therapy (THRT)—commonly used for hypothyroidism—may unintentionally fuel tumor growth and reduce the efficacy of anti-estrogen treatments in SR+ breast cancer patients by upregulating key cell cycle drivers.
Results in Context
- Impact on Proliferation (S-Phase):
The study found that TH alone, or in combination with E2, significantly increased the percentage of breast cancer cells in the S-phase (the phase of the cell cycle where DNA is replicated).
- Context: An increase in the S-phase fraction indicates active and aggressive cell division. In mouse models (in vivo), tumors treated with E2 + TH were significantly larger and showed higher expression of Ki-67 (a clinical marker of proliferation) compared to those treated with E2 alone.
- Thyroxine-Induced Tamoxifen Resistance:
A critical finding regarding risk is the interaction with tamoxifen. In the presence of TH, the study observed that tamoxifen—normally an estrogen antagonist (blocker)—shifted toward functioning as a partial agonist, effectively promoting cell viability rather than inhibiting it.
- Statistical Note: The combination of Tamoxifen + TH resulted in the highest cell viability and lowest apoptosis rates in MCF7 cells compared to controls.
- Molecular Mechanism (Biomarkers):
The study utilized RNA-seq to identify that the combination of TH and E2 upregulates critical cell cycle regulatory genes, specifically E2F1, MYC, and various cyclins (CCNA, CCNB, CCND1).
- Biomarker Definition: These genes act as accelerators for cell division. Their upregulation provides a mechanistic explanation for why thyroid hormone might worsen outcomes in hormone-dependent cancers.
Assertive Critical Appraisal
- Appraisal of Biomarker Claim (Mechanistic Plausibility):
The authors successfully establish a biological plausibility for the epidemiological observation that hyperthyroidism or THRT increases breast cancer risk. By isolating the effects of T4 and T3 on SR+ cell lines, they confirm that this risk is mediated through specific estrogenic crosstalk pathways.
- Critique: It is important to note that this is a pre-clinical study using cell lines and xenograft mice. While the mechanisms are robustly defined, the direct translation to human clinical risk stratification requires caution. However, the study validates prior clinical observations made by this group regarding poor outcomes in SR+ patients on THRT.
- Specificity of Risk:
The study explicitly demonstrates that these pro-carcinogenic effects are limited to Steroid Receptor-positive (SR+) cells (e.g., MCF7, T47D). SR-negative cell lines (e.g., MDA-MB-468) did not show enhanced proliferation with TH treatment. This is a crucial distinction for clinicians, suggesting that “thyroxine risk” is not universal to all breast cancers but specific to the hormonal subtype. - Reporting Quality (REMARK/Pre-clinical):
The reporting of molecular methods is high quality. The authors utilized authenticated cell lines and patient-derived xenografts (PDX), which offer a more clinically relevant model than standard cell cultures. However, the study does not account for the complex immune system interactions that would occur in a human patient, which could modulate these risks.
Applicability
These findings are highly applicable to the management of post-menopausal women with SR+ breast cancer who are also being treated for hypothyroidism. The data suggests that aggressive TSH suppression (resulting in high circulating T4) might be counterproductive in this specific patient population. It also supports the hypothesis that fulvestrant (a full ER degrader) may be a superior therapeutic choice over tamoxifen for patients with high thyroid hormone levels, as fulvestrant maintained efficacy in the presence of TH while tamoxifen did not.
Research Objective
To define the molecular and biological changes, as well as hormonal and treatment interactions, between estrogenic and thyroid hormones that drive proliferation in breast cancer.
Study Design
- Design: Pre-clinical mechanistic study utilizing in vitro (cell culture) proliferation/apoptosis assays and in vivo (mouse xenograft) tumor growth models.
- Key Interventions: Treatment with Thyroid Hormone (T3/T4), Estrogen (E2), Tamoxifen, and Fulvestrant (ICI).
Setting and Participants
- Setting: Laboratory (University of Colorado Anschutz Medical Campus).
- Models: Human breast cancer cell lines (MCF7, T47D, MDA-MB-468, SKBR3) and female NOD-SCID-gamma (NSG) mice implanted with UCD12 patient-derived xenografts.
Bibliographic Data
- Title: Thyroid hormone enhances estrogen-mediated proliferation and cell cycle regulatory pathways in steroid receptor-positive breast Cancer
- Authors: Wahdan-Alaswad RS, Edgerton SM, Kim HM, Tan AC, Haugen BR, Liu B, Thor AD
- Journal: Cell Cycle
- Year: 2024 (Published online 2023)
- DOI: 10.1080/15384101.2023.2249702
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.