
Comment:
Although conventional treatments for breast cancer has made astounding improvements over the 35 years that I’ve been in the field, we have to acknowledge that along with it comes a long-term price paid by the patient’s systemic health. This study provides a definitive signal on the iatrogenic risks associated with the standard-of-care.
The clinical reality is that the conventional tools demonstrate efficacy for their specific indication ( the cancer), but introduce significant structural harms that manifest decades later. This is most evident in the elevated risk of lung, esophageal, and kidney cancers in deprived populations, where the intersection of treatment and lifestyle factors creates a significant survival hazard. As Naturopathic Doctors, we understand that cancer survivorship is not a return to baseline, however the magnitude of the risk is surprising.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
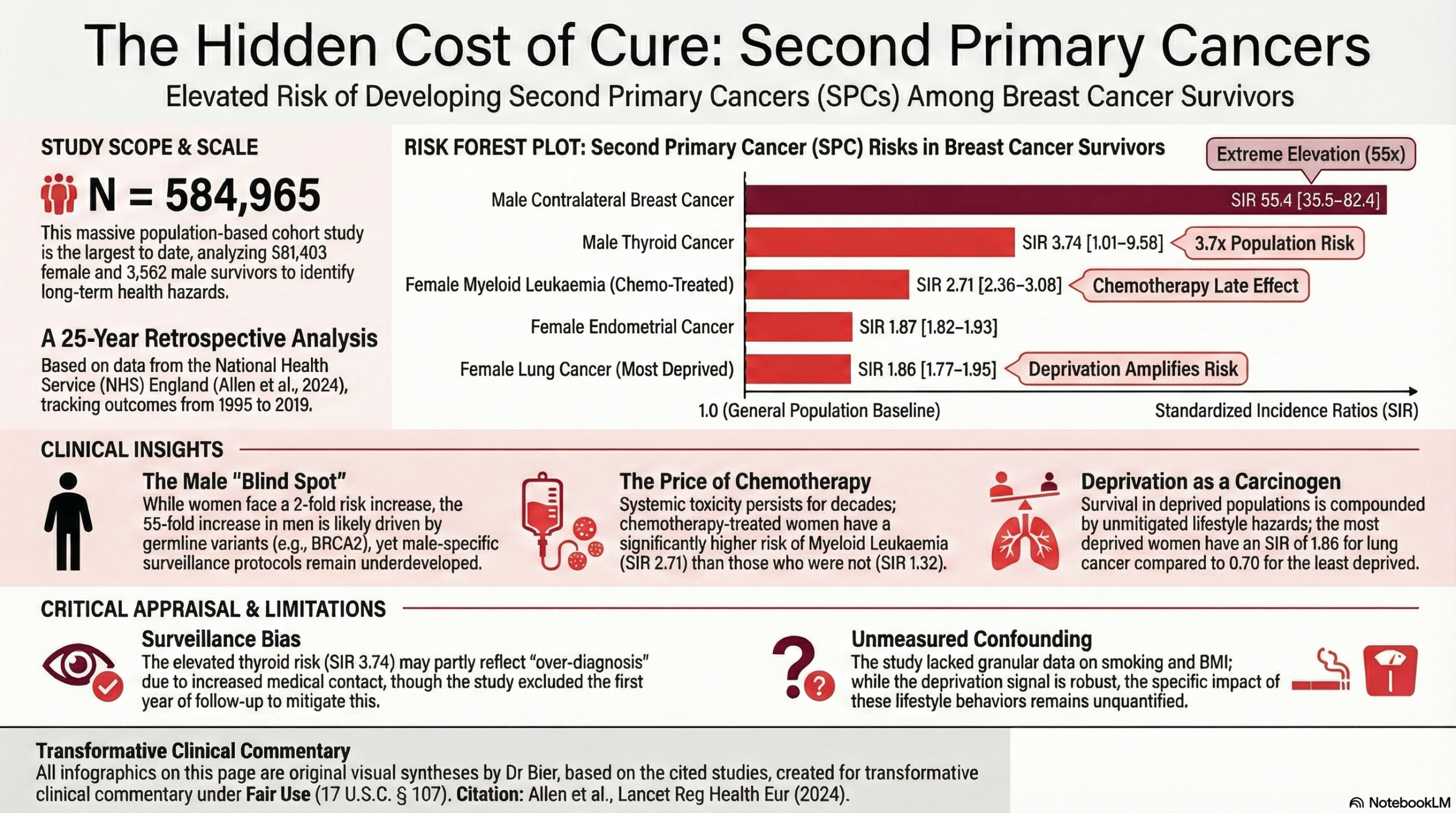
This massive population-based cohort study—the largest of its kind—demonstrates that survivors of both female and male breast cancer (BC) face a significantly higher risk of developing second primary cancers (SPCs) compared to the general population. Key takeaways include a staggering 55-fold increase in contralateral breast cancer risk for men and a 2-fold increase for women. Crucially, the study identifies socioeconomic deprivation as a novel and significant risk factor for non-breast SPCs in women, likely driven by lifestyle factors such as smoking and obesity. While relative risks are highest in those diagnosed before age 50, absolute cumulative risks are higher in older survivors, suggesting that long-term, multi-organ surveillance is warranted across all age groups.
Results in Context
Main Results
- Female Survivors: Overall SPC risk was 25% higher than the general population (SIR: 1.25). Non-breast SPC risk was elevated by 10% (SIR: 1.10).
- Male Survivors: Overall SPC risk was 15% higher (SIR: 1.15). Non-breast SPC risk was also elevated by 10% (SIR: 1.10).
- Specific Elevated Risks: Significant elevations were found for the contralateral breast, endometrium, ovary, and prostate.
- Definitions: Standardized Incidence Ratio (SIR) is the ratio of observed SPC cases in the cohort to the number of cases expected in the general population. An SIR of 2.02 means the cohort had 2.02 times the risk of the general population.
Key Associations
- Deprivation: Females in the most deprived quintile had a 34% higher risk of non-breast SPCs compared to the general population, while those in the least deprived quintile had no elevated risk (SIR: 1.00).
- Age at Diagnosis: Relative risks for non-breast SPCs were higher for those diagnosed with BC under age 50 (SIR: 1.34) versus age 50 or over (SIR: 1.07).
- Treatment Effects: In females, radiotherapy was associated with a 7% increase in non-breast SPC risk. Chemotherapy was strongly associated with myeloid leukaemia (SIR: 2.71). Hormonal therapy was protective against contralateral breast cancer (HR: 0.90) but increased endometrial cancer risk (HR: 1.09).
- Tumour Biology: ER-positive (HR: 0.93) and HER2-positive (HR: 0.88) status were associated with lower non-breast SPC risks compared to receptor-negative disease.
Participants
- The final cohort included 581,403 females and 3,562 males diagnosed with invasive BC between 1995 and 2019.
- A total of 52,620 SPCs were diagnosed in females and 504 in males.
Assertive Critical Appraisal
Limitations & Bias (STROBE Framework)
- Unmeasured Confounding: The primary limitation is the lack of data on smoking status, BMI, and alcohol intake. The authors hypothesize these factors drive the deprivation-associated risks, but this remains unproven within this dataset.
- Genetic Data Gap: Data on germline mutations (e.g., BRCA1/2) were unavailable. This likely explains the high relative risks in younger patients, but the study cannot quantify this contribution.
- Surveillance Bias: Survivors are under regular medical review, which may lead to earlier or more frequent detection of second cancers compared to the general population. The authors mitigated this by starting follow-up one year after the initial BC diagnosis.
Reporting Quality Assessment (STROBE)
- Confounding Efforts: The authors provide a robust description of efforts to address confounding, using multivariable Cox proportional hazards models adjusted for age, year of diagnosis, ethnicity, deprivation, tumour characteristics, and treatments.
- Censoring Precision: A major strength is the explicit accounting for prophylactic/curative surgeries (e.g., bilateral salpingo-oophorectomy) in the censoring process, which prevents underestimation of risk at those specific sites.
Reporting Quality Assessment (RECORD) for RWE
- Data Sourcing: The study excels in its description of data sources, utilizing the National Cancer Registration Dataset (NCRD) with 98-99% complete case ascertainment linked to Hospital Episode Statistics (HES).
- Validation: The use of a novel linkage of National Disease Registration Service datasets allows for high-fidelity longitudinal tracking.
Applicability
- The findings are highly generalizable to BC survivors in developed healthcare systems. The identification of high-risk subgroups (younger patients, those with receptor-negative disease, and those from deprived areas) provides a clear framework for personalized risk stratification.
Research Objective
To estimate site-specific relative and absolute risks of second primary cancers (SPCs) in a large cohort of male and female breast cancer survivors and to assess how these risks vary by sociodemographic, tumour, and treatment factors.
Study Design
This was a retrospective cohort study using population-scale linked electronic health records from the National Health Service (NHS) England.
Setting and Participants
- Setting: England, United Kingdom, with data covering 1995 to 2019.
- Eligibility: Patients diagnosed with a first primary invasive BC during the study period, excluding those with stage 0 (non-invasive), stage 4 (metastatic), or unknown stage. Patients were followed from 365 days post-diagnosis until death, emigration, SPC diagnosis, or the end of 2020.
Bibliographic Data
- Title: Risks of second primary cancers among 584,965 female and male breast cancer survivors in England: a 25-year retrospective cohort study
- Authors: Isaac Allen, Hend Hassan, Andrew Bacon, Craig Knott, Diana Eccles, Eva J. A. Morris, et al.
- Journal: The Lancet Regional Health – Europe
- Year: 2024
- DOI: https://doi.org/10.1016/j.lanepe.2024.100903
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.