
Comment:
With the caveat that this is an abstract and not the full study, this trial is a crucial validation of the “less is more” principle that come up frequently. The significant improvement in Time to Treatment Failure (TTF) with the Fixed-Dose (7/7) schedule confirms what proponents of metronomic chemotherapy have argued for years: the Maximum Tolerated Dose (MTD) is rarely the Optimal Biological Dose.
Much like the metronomic regimens I have reviewed previously, this 7/7 schedule succeeds not by hitting the tumor harder, but by allowing the patient to actually sustain the treatment. The standard 14-day dosing frequently leads to “forced de-escalation” via dose interruptions or discontinuations due to severe Hand-Foot Syndrome and GI toxicity.
By capping the “on” phase at 7 days—the point where mathematical models suggest the cytotoxic benefit plateaus—we maintain efficacy while preserving the patient’s quality of life. The concept of metronomic chemotherapy is not one I’ve found most oncologist are aware of or comfortable with, so this may be a good option to present.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
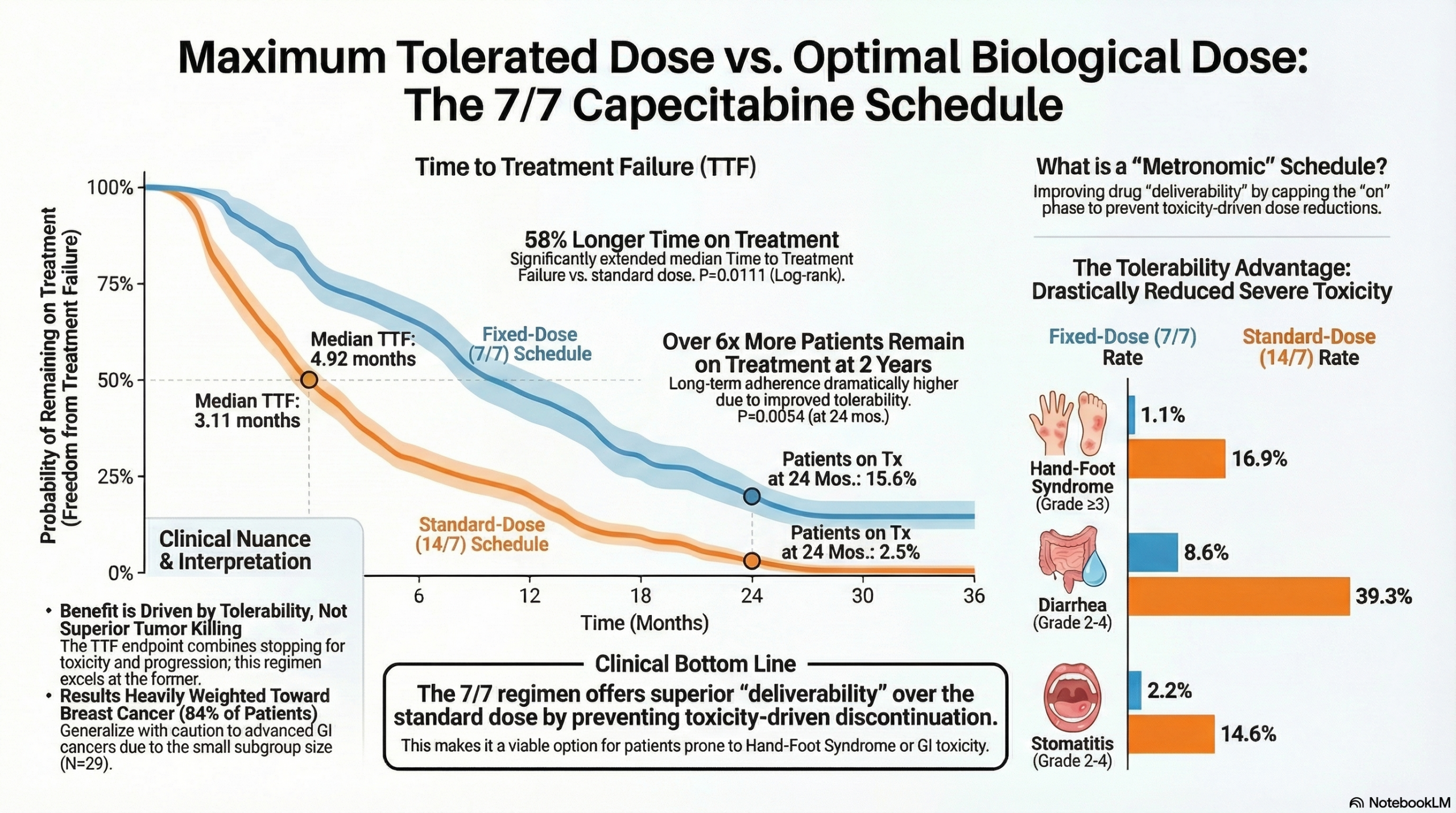
This randomized trial suggests that a “Fixed-Dose” (FD) capecitabine regimen (1500 mg BID, 7 days on, 7 days off) offers a superior Time to Treatment Failure (TTF) and significantly reduced severe toxicity compared to the FDA-approved “Standard Dose” (SD) (1250~mg/m^{2} BID, 14 days on, 7 days off) in patients with metastatic breast (MBC) and advanced GI cancers. While the results argue strongly for the improved tolerability of the FD regimen, clinicians should interpret the Time to Treatment Failure (TTF) endpoint carefully; it is a composite measure influenced by both disease progression and toxicity-related discontinuation. Therefore, the superiority of the FD arm may be driven primarily by patients staying on the drug longer due to fewer side effects, rather than superior tumor shrinkage.
Results in Context
Primary Outcome: Time to Treatment Failure (TTF)
- The median TTF was significantly longer in the Fixed Dose (FD) arm compared to the Standard Dose (SD) arm.
- FD Arm: 4.92 months (95% CI: 3.02, 5.93).
- SD Arm: 3.11 months (95% CI: 2.49, 3.90).
- Statistical Significance: Log-rank P=0.011.
- Definition: Time to Treatment Failure (TTF) measures the time from randomization to discontinuation of treatment for any reason, including disease progression, treatment toxicity, or death.
Landmark Analysis: Freedom from Treatment Failure (FFTF)
- At 24 months, the proportion of patients remaining on treatment (Freedom from Treatment Failure) was significantly higher in the FD arm.
- FD Arm: 15.6%.
- SD Arm: 2.5%.
- P-value: 0.005.
Key Secondary Outcomes: Harms and Adverse Events
The study reports a significant reduction in severe toxicities with the FD regimen. The Standard Dose arm was associated with higher rates of Grade 3+ adverse events.
- Hand-Foot Syndrome (HFS):
- Grade \ge 3: 1.08% in the FD arm vs. 16.9% in the SD arm (P=0.0002).
- Diarrhea:
- Grade \ge 3: 0.0% in the FD arm vs. 6.7% in the SD arm (P=0.0125).
- Grade 2-4: 8.6% in the FD arm vs. 39.3% in the SD arm (P<0.0001).
- Grade \ge 3: 1.08% in the FD arm vs. 16.9% in the SD arm (P=0.0002).
- Stomatitis:
- Grade \ge 3: 0.0% in the FD arm vs. 22.5% in the SD arm (P<0.0001)—Note: The table lists 22.5% for Grade \ge 3, but this number appears in the Grade \ge 3 row under Diarrhea in one column and Stomatitis in another, suggesting potential formatting alignment issues in the source table. The text, however, confirms toxicities were “more common in SD”.
Assertive Critical Appraisal
Risk of Bias (RoB 2 Framework)
- Judgment: Some Concerns.
- Methodological Limitations: As this source is a conference poster/abstract, full methodological details regarding allocation concealment and blinding are absent.
- Blinding: The trial compares a 7/7 schedule vs. a 14/7 schedule. Unless placebo pills were used to mask the “off” week in the SD arm, this trial was likely open-label. Knowledge of the assigned arm could influence patient reporting of subjective symptoms (like fatigue or nausea) and clinician decisions to discontinue treatment, potentially biasing the TTF endpoint.
Critical Analysis of the Endpoint (TTF)
- Composite Nature: The primary endpoint, Time to Treatment Failure, is a composite of efficacy (progression) and tolerability (toxicity). Since standard-dose capecitabine is notoriously difficult to tolerate, patients in the SD arm are more likely to quit due to toxicity. This “failure” counts the same as cancer progression.
- Interpretation: The significant improvement in TTF for the FD arm confirms it is more deliverable and better tolerated. However, it does not definitively prove it kills cancer cells better than the standard dose, though the authors note that a previous report on the MBC cohort showed similar progression-free survival (PFS) and overall survival (OS).
Data Discrepancy Note
- There is a discrepancy between the text summary and the provided data table regarding Grade 2-4 Hand-Foot Syndrome (HFS).
- The text states: “Grade 2 and higher toxicities were more common in SD compared to FD, including HFS”.
- The table reports: HFS Grade 2-4 as 44.9% for FD vs. 14.0% for SD.
- Appraisal: This tabular data contradicts the narrative conclusion for Grade 2 HFS. However, the Grade \ge 3 (severe) HFS data clearly favors the FD arm (1.08% vs 16.9%). Clinicians should prioritize the Grade 3+ data as it represents the clinically dose-limiting toxicity.
Applicability and Population
- Imbalance in Cohorts: The study enrolled 182 patients: 153 with Metastatic Breast Cancer (MBC) and only 29 with advanced GI cancers. The conclusions are heavily weighted toward the breast cancer population. Caution should be used when generalizing these findings to GI cancer patients due to the small sample size (N=29) in that subgroup.
- Real-World Relevance: Despite the limitations, the Fixed Dose (7 days on, 7 days off) is a highly relevant strategy for clinicians managing patients who struggle with the toxicity of the standard FDA-approved 14-day regimen.
Reporting Quality Assessment (CONSORT)
- Missing Information: Being a poster presentation, the document lacks a participant flow diagram and detailed statistical analysis plans (e.g., handling of missing data), which are standard requirements for a full CONSORT-compliant publication.
Study Details
Research Objective
To compare Time to Treatment Failure (TTF) and toxicity profiles between standard-dose (SD) and fixed-dose (FD) capecitabine in patients with metastatic breast cancer (MBC) and advanced gastrointestinal (GI) cancers.
Study Design
- Type: Randomized Controlled Trial (RCT).
- Allocation: Randomized 1:1.
- Intervention:
- FD Arm: Capecitabine 1500 mg orally twice daily, 7 days on, 7 days off (FD-7/7).
- SD Arm: Capecitabine 1250~mg/m^{2} orally twice daily, 14 days on, 7 days off (SD-14/7).
Setting and Participants
- Setting: Multi-center (University of Kansas Cancer Center and affiliated sites).
- Participants: N=182 total.
- N=153 Metastatic Breast Cancer (MBC).
- N=29 Advanced GI cancers (colorectal, small bowel, gastroesophageal, pancreatic, bile duct).
Bibliographic Data –
Title: Standard-dose vs fixed-dose capecitabine in patients with advanced gastrointestinal and metastatic breast cancer.
Authors: Gvazava N, Khan QJ, Clark L, et al.
Journal: Journal of Clinical Oncology (ASCO Poster Session).
Year: 2025 (Copyright), May 28, 2025.
DOI: 10.1200/JCO.2025.43.16_suppl.109
Original Article:
Full text pdf: here.
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.