
Comment:
This study complicates the de-escalation narrative we see surrounding radiation for breast cancer. While randomized trials have proven we can omit radiation in low-risk settings, this data suggests that ‘real-world’ safety may be lower than trial safety. This may be because the registry included patients with higher tumor burdens (up to T2/N1) and unmeasured frailty (selection bias) that wouldn’t have qualified for trials like PRIME II. It forces us to ask whether we applying ‘low-risk’ omission strategies too broadly to patients who actually have intermediate-risk factors, or is this study giving skewed data due to the patient selection?
Audio Overview
Summary:
Clinical Bottom Line
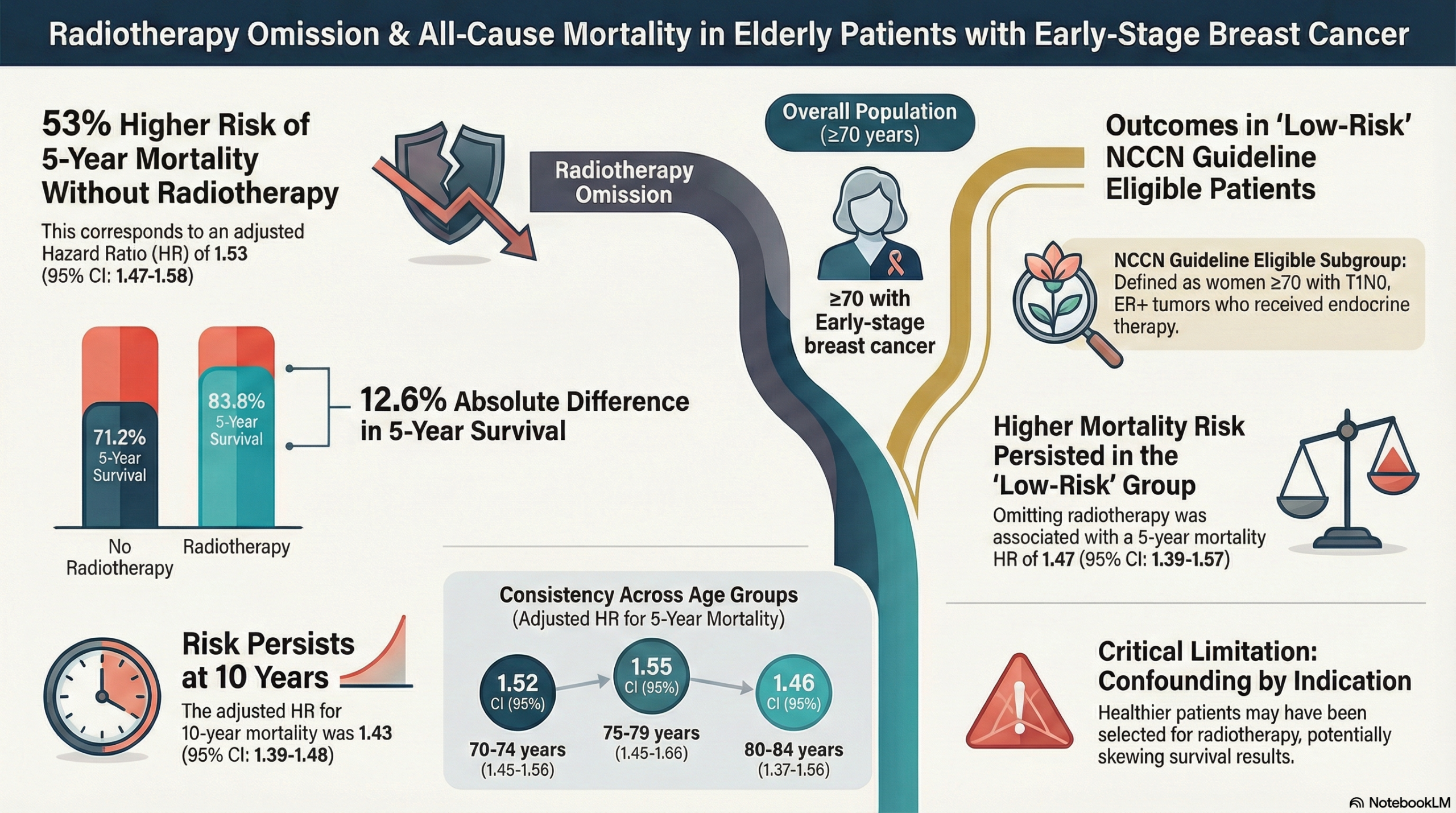
This large-scale observational study challenges current “de-escalation” guidelines which suggest radiotherapy (RT) can be safely omitted in low-risk elderly women. The authors found a strong, statistically significant association between omitting RT and increased overall mortality in women aged \ge70, even among those meeting NCCN “low-risk” criteria (T1N0, ER+, receiving endocrine therapy). However, you must interpret these findings with significant caution. Because this is registry data (NCDB) lacking information on cause of death or recurrence, it is impossible to determine if the increased mortality was driven by breast cancer or by selection bias (i.e., healthier women were selected for radiation, while frail women were not).
Results in Context
Primary Outcome: Overall Survival (OS)
The study focused exclusively on all-cause mortality, as cancer-specific death is not recorded in the NCDB.
- Main Result: Patients who did not receive radiotherapy had a significantly higher mortality rate compared to those who did.
- Unadjusted 5-year survival: 71.2% (No RT) vs 83.8% (RT).
- Absolute Difference: There was a 12.6% absolute survival difference at 5 years favoring radiotherapy.
- Adjusted Hazard Ratios (HR): After adjusting for clinical factors (age, stage, comorbidities), the risk of death remained significantly higher for women omitting RT:
- 3-year mortality: HR 1.65 (95% CI: 1.57-1.72).
- 5-year mortality: HR 1.53 (95% CI: 1.47-1.58).
- 10-year mortality: HR 1.43 (95% CI: 1.39-1.48).
- Definition: A Hazard Ratio (HR) of 1.53 implies that at any point in time during the study, women who did not receive radiation were 53% more likely to die than those who did.
Subgroup Analysis: NCCN Guideline Eligible Patients
The authors analyzed the specific subgroup of women who meet current criteria for RT omission (Age \ge70, T1N0, ER+, receiving endocrine therapy).
- Result: Even in this “low-risk” group, omitting RT was associated with higher mortality.
- 5-year mortality: HR 1.47 (95% CI: 1.39-1.57).
- Absolute Difference: 10.3% survival difference at 5 years (77.4% vs 87.7%).
Assertive Critical Appraisal
Limitations & Bias (STROBE/RECORD Framework)
- Critical Data Gap (Cause of Death): This is the study’s most significant flaw. The NCDB does not provide cause of death or recurrence data. Consequently, we cannot know if the survival benefit is due to better cancer control or simply because patients chosen for radiation were healthier at baseline. The authors admit this limitation prevents evaluating breast-cancer-specific survival.
- Selection Bias (Confounding by Indication): In real-world practice, clinicians often omit RT for patients with poor performance status or severe comorbidities. While the authors adjusted for Charlson comorbidity scores and age, observational adjustments rarely fully capture patient “frailty.” The survival curves separate very early (within 1 year), suggesting that patients in the “No RT” group may have had higher baseline mortality risks unrelated to breast cancer.
- Adherence Data Missing: The study assumes patients received endocrine therapy if prescribed, but adherence rates in the real world are often poor. If the “No RT” group also had lower adherence to endocrine therapy, their mortality would be artificially inflated.
Reporting Quality Assessment (STROBE)
- Strengths: The study utilizes a massive sample size (N=115,516), providing high statistical power compared to the smaller randomized trials (CALGB 9343, PRIME II) often cited in guidelines. The authors transparently report propensity score-weighted analyses to attempt to correct for selection bias.
- Weaknesses: The inability to distinguish between cancer recurrence and other causes of death fundamentally limits the clinical applicability of the findings regarding cancer treatment efficacy.
Applicability
This study reflects “real-world” outcomes rather than controlled trial settings. However, the conflict between these findings (RT improves survival) and randomized trials like CALGB 9343 (RT does not improve survival, only local control) suggests that in routine practice, patient selection plays a massive role. Clinicians should use this data to be cautious about omitting RT in healthy 70-year-olds, but it does not definitively prove RT prevents death in this population.
Research Objective
To evaluate the influence of post-BCS radiotherapy on overall survival among elderly patients (\ge70 years) who received breast-conserving surgery for early-stage breast cancer, utilizing national registry data to address gaps left by smaller clinical trials.
Study Design
- Design: Retrospective, observational cohort study.
- Data Source: National Cancer Database (NCDB), covering \sim 70% of newly diagnosed cancer cases in the US.
- Analysis: Kaplan-Meier survival analysis, Multivariable Cox proportional hazards models, and Propensity score-weighted analysis.
Setting and Participants
- Population: 115,516 women aged ≥70 years diagnosed between 2004 and 2014.
- Inclusion Criteria:
- T1-2 N0-1 M0 breast cancer.
- Treated with Breast-Conserving Surgery (BCS).
- Groups:
- Received Radiotherapy: 84,710 (73.3%).
- Did Not Receive Radiotherapy: 30,806 (26.7%).
Bibliographic Data
- Title: Radiotherapy after breast-conserving surgery for elderly patients with early-stage breast cancer: A national registry-based study
- Authors: Wang F, Meszoely I, Pal T, Mayers IA, Bailey CE, Zheng W, Shu XO
- Journal: Int. J. Cancer
- Year: 2021
- DOI: 10.1002/ijc.33265
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.