
Comment:
This study again reinforces that we need to view blood sugar through the lens of oncologic outcome. Hyperglycemia is a driver of cancer recurrence, so modulating sugar intake during chemotherapy is a low-toxicity, low-cost strategy that somehow is still controversial despite all the research supporting it. Since sugar consumption is the primary lever for these glucose excursions, this suggests ‘metabolic management’ should be standard practice in the adjuvant setting—transforming diet from a lifestyle suggestion into a verifiable safety parameter.
The Wonk Debate – Audio Critique & Clinical Commentary:
Summary:
Clinical Bottom Line
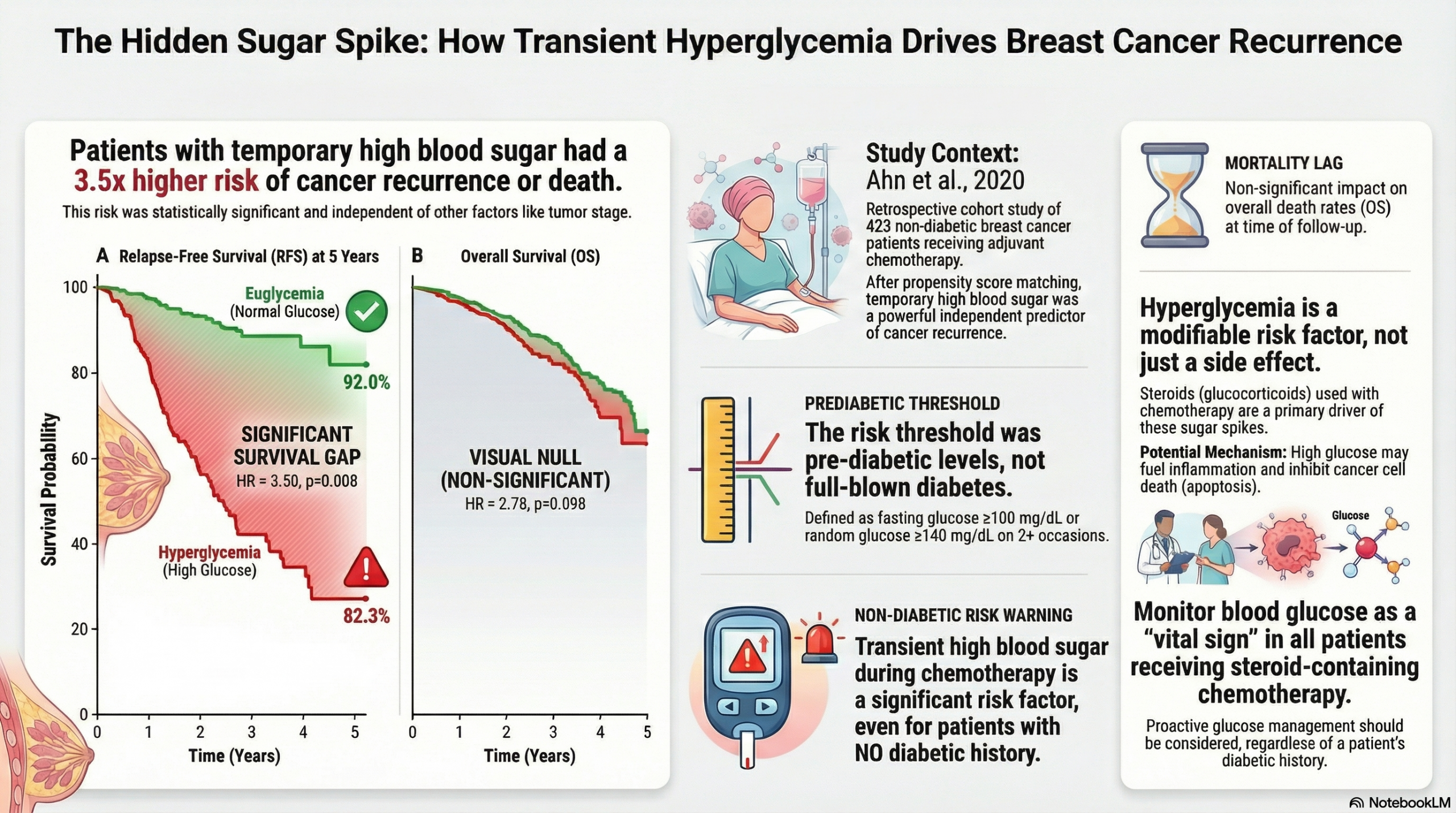
This retrospective cohort study identifies hyperglycemia during adjuvant chemotherapy as a significant, independent prognostic factor for reduced Relapse-Free Survival (RFS) in breast cancer patients with no prior history of diabetes. While the study demonstrates a strong association between transient hyperglycemia and recurrence (Hazard Ratio ~3.5), it did not find a statistically significant impact on Overall Survival (OS), likely due to the low number of mortality events during the follow-up period. Clinicians should be aware that glucocorticoid-induced hyperglycemia in non-diabetic patients is not merely a transient metabolic side effect but a potential marker for poorer oncologic outcomes.
Results in Context
Main Results
- Prevalence: Among 423 non-diabetic patients receiving adjuvant chemotherapy (all regimens included glucocorticoids), 19.4% developed hyperglycemia.
- Primary Outcome (Relapse-Free Survival – RFS): In the Propensity Score Matched (PSM) analysis, hyperglycemia was an independent prognostic factor for RFS.
- Hazard Ratio (HR): 3.504 (95% CI: 1.390–8.836; $p=0.008$).
- Interpretation: Patients who experienced hyperglycemia had a risk of recurrence or death approximately 3.5 times higher than those who maintained euglycemia.
- 5-Year RFS Rates: 82.3% in the hyperglycemia group vs. 92.0% in the euglycemia group ($p=0.011$).
- Secondary Outcome (Overall Survival – OS): The study failed to demonstrate a significant difference in OS.
- Hazard Ratio: 2.775 (95% CI: 0.828–9.308; $p=0.098$).
- 5-Year OS Rates: 92.0% (hyperglycemia) vs. 94.6% (euglycemia) ($p=0.113$).
Definitions & Context
- Hyperglycemia Definition: Defined strictly as fasting plasma glucose $\ge100~mg/dL$ or random blood glucose $\ge140~mg/dL$ during 2 or more cycles of chemotherapy. This threshold aligns with “prediabetes” criteria, highlighting that even mild dysglycemia was associated with worse outcomes.
- Propensity Score Matching (PSM): The authors matched patients 1:1 based on age, sentinel lymph node biopsy, total steroid dosage, nodal stage, hypertension, and BMI to reduce confounding.
Assertive Critical Appraisal
Limitations & Bias (STROBE Framework)
- Measurement Bias (High Concern): Blood glucose was measured only once in the morning on the day of chemotherapy. This sporadic sampling likely underestimates the true incidence of hyperglycemia, particularly post-prandial spikes or acute steroid-induced hyperglycemia that occurs 6–8 hours after administration. The “euglycemia” group may effectively contain patients with undetected hyperglycemia.
- Retrospective Design: As a single-institution retrospective study, the findings are subject to selection bias and limited generalizability.
- Lack of Intervention Data: The study did not record whether hyperglycemic patients received insulin or oral hypoglycemic agents. If untreated hyperglycemia drives tumor proliferation (via insulin/IGF-1 pathways), the lack of treatment data obscures whether correcting the glucose would reverse the risk.
Reporting Quality Assessment (STROBE)
- Confounding Variables: The authors adequately utilized Propensity Score Matching (PSM) to balance key covariates like BMI and steroid dosage. This strengthens the validity of the comparison, though unmeasured confounders (e.g., diet, baseline insulin resistance) remain a risk.
- Biologic Plausibility: The authors provide a sound rationale for the findings, citing mechanisms where hyperglycemia increases pro-inflammatory factors (IL-6, TNF-a) and inhibits p53 apoptotic activity, potentially fostering a pro-tumorigenic environment.
Applicability
This study is highly relevant for general oncologists and primary care clinicians. It suggests that glucose monitoring in breast cancer patients should not be limited to those with established diabetes. The data supports considering “chemotherapy-induced hyperglycemia” as a modifiable risk factor.
Research Objective
The study aimed to investigate the effect of hyperglycemia occurring during adjuvant chemotherapy on the prognosis (specifically Relapse-Free Survival and Overall Survival) of breast cancer patients without a known history of diabetes.
Study Design
- Type: Retrospective Cohort Study with Propensity Score Matching.
- Timeframe: Patients underwent surgery between January 2010 and December 2015.
- Follow-up: Median follow-up period was 70.1 months.
Setting and Participants
- Setting: Department of Surgery, Jeonbuk National University Hospital, Korea.
- Inclusion: 423 patients included in the initial analysis (matched cohort: 75 pairs, n=150).
- Key Characteristics: All patients were female, mean age $47.4 \pm 7.7$ years.
- Exclusions: Patients with preexisting diabetes mellitus, those who did not receive chemotherapy, or those receiving chemotherapy without glucocorticoids.
Bibliographic Data
- Title: Hyperglycemia during Adjuvant Chemotherapy as a Prognostic Factor in Breast Cancer Patients without Diabetes
- Authors: Ha Rim Ahn, Sang Yull Kang, Hyun Jo Youn, Sung Hoo Jung
- Journal: Journal of Breast Cancer
- Year: 2020
- DOI: 10.4048/jbc.2020.23.e44
Original Article:
Full text: PubMed Central
Fair Use & Copyright: This post provides a transformative, thesis‑driven critical appraisal intended for educational and scholarly purposes. It is not a reproduction of, nor a market substitute for, the original research article.
Support the Version of Record: To support the copyright holders and verify the underlying data—including primary survival curves, risk estimates, and other core outcomes—readers are strongly encouraged to access the original Version of Record via the link or DOI provided above.
Medical Disclaimer: This content is for informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment.